Articles
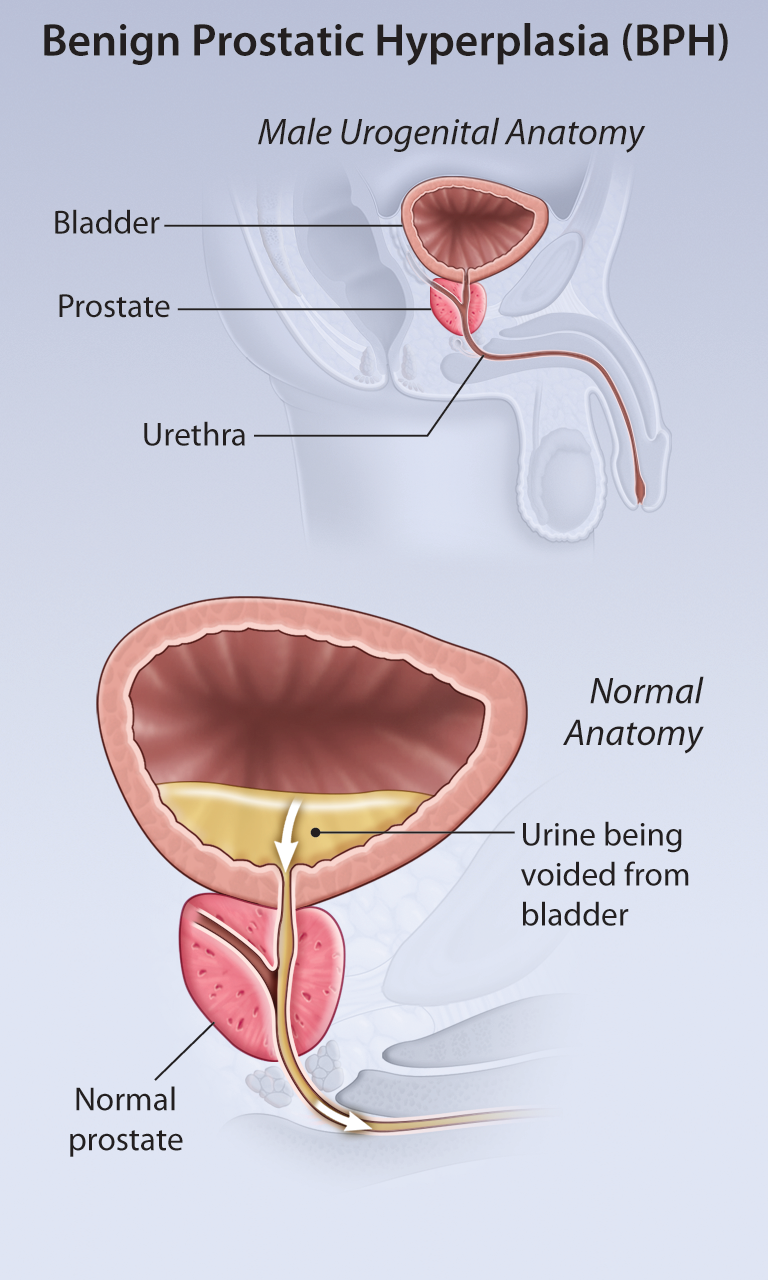
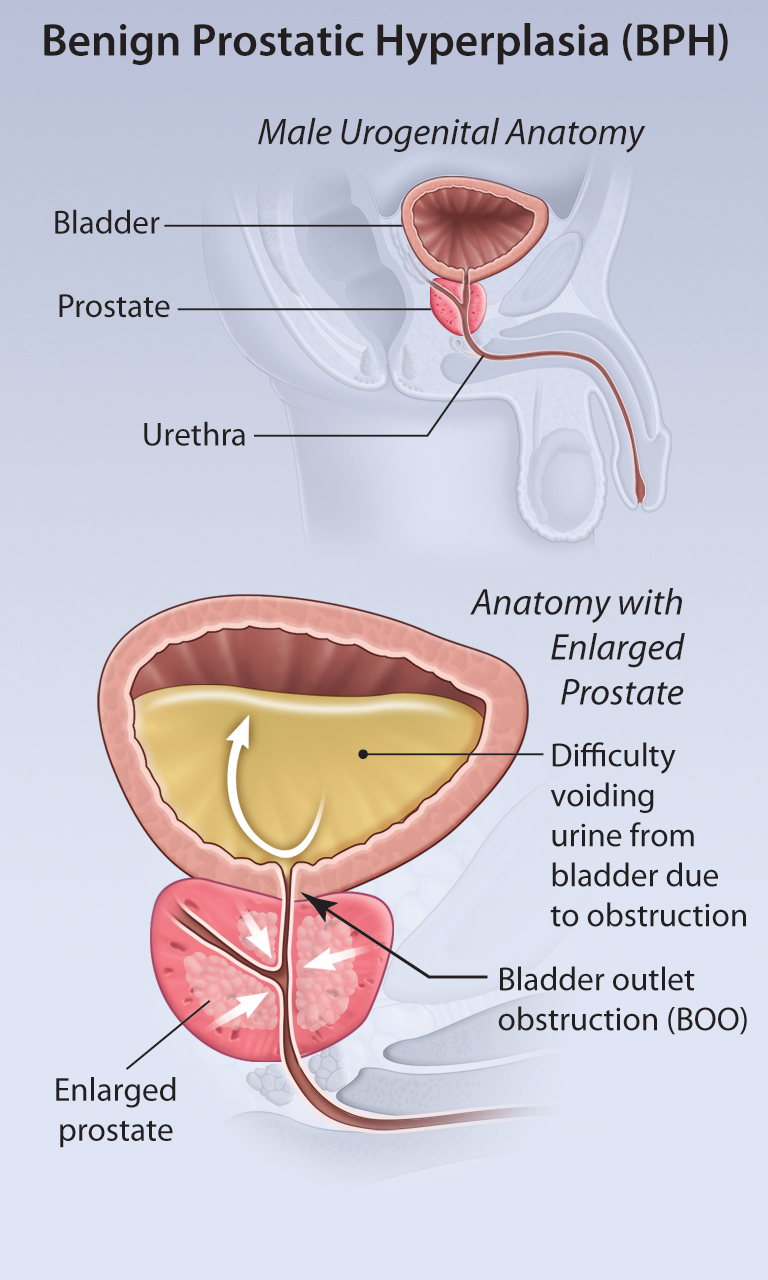
Benign Prostatic Hyperplasia—Medical and Surgical Treatment Options
Benign Prostatic Hyperplasia—Medical and Surgical Treatment Options

Geriatrics: Patient Education
Geriatrics: Patient Education
Coming Soon...
- Read more about Geriatrics: Patient Education
- Log in or register to post comments
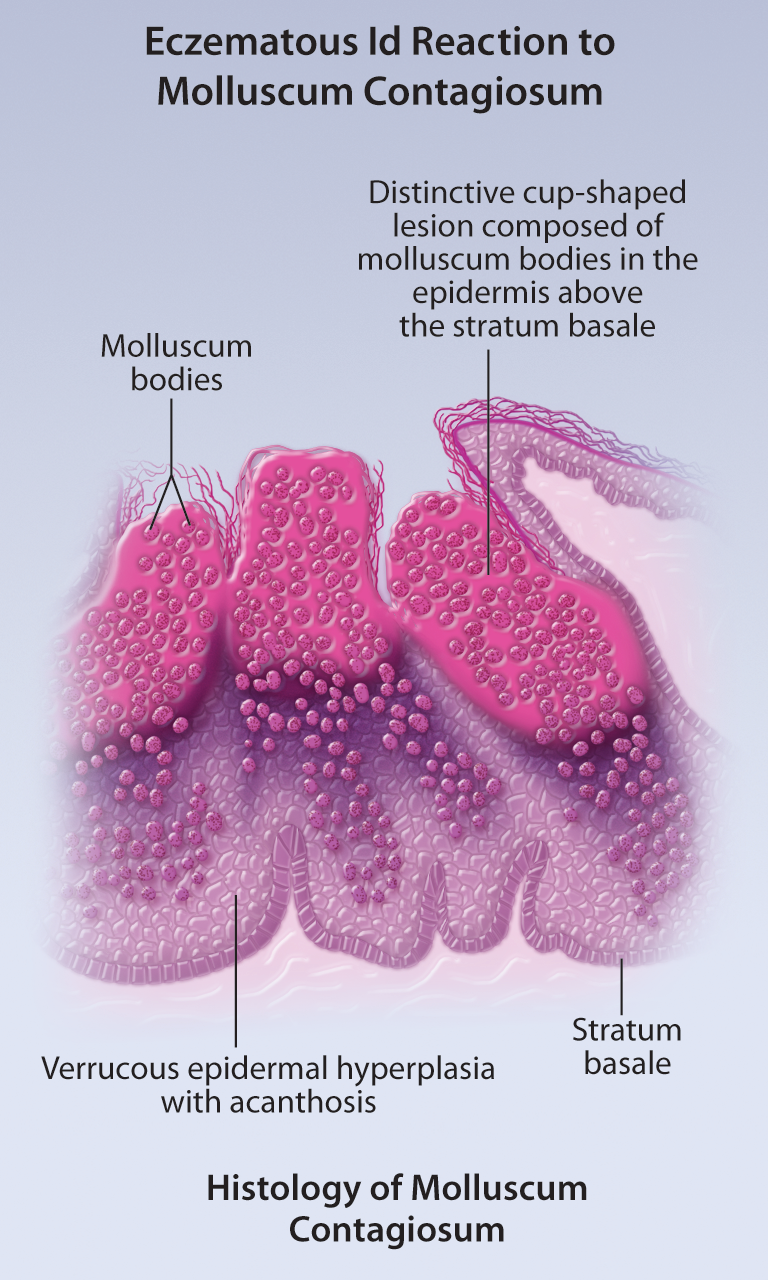
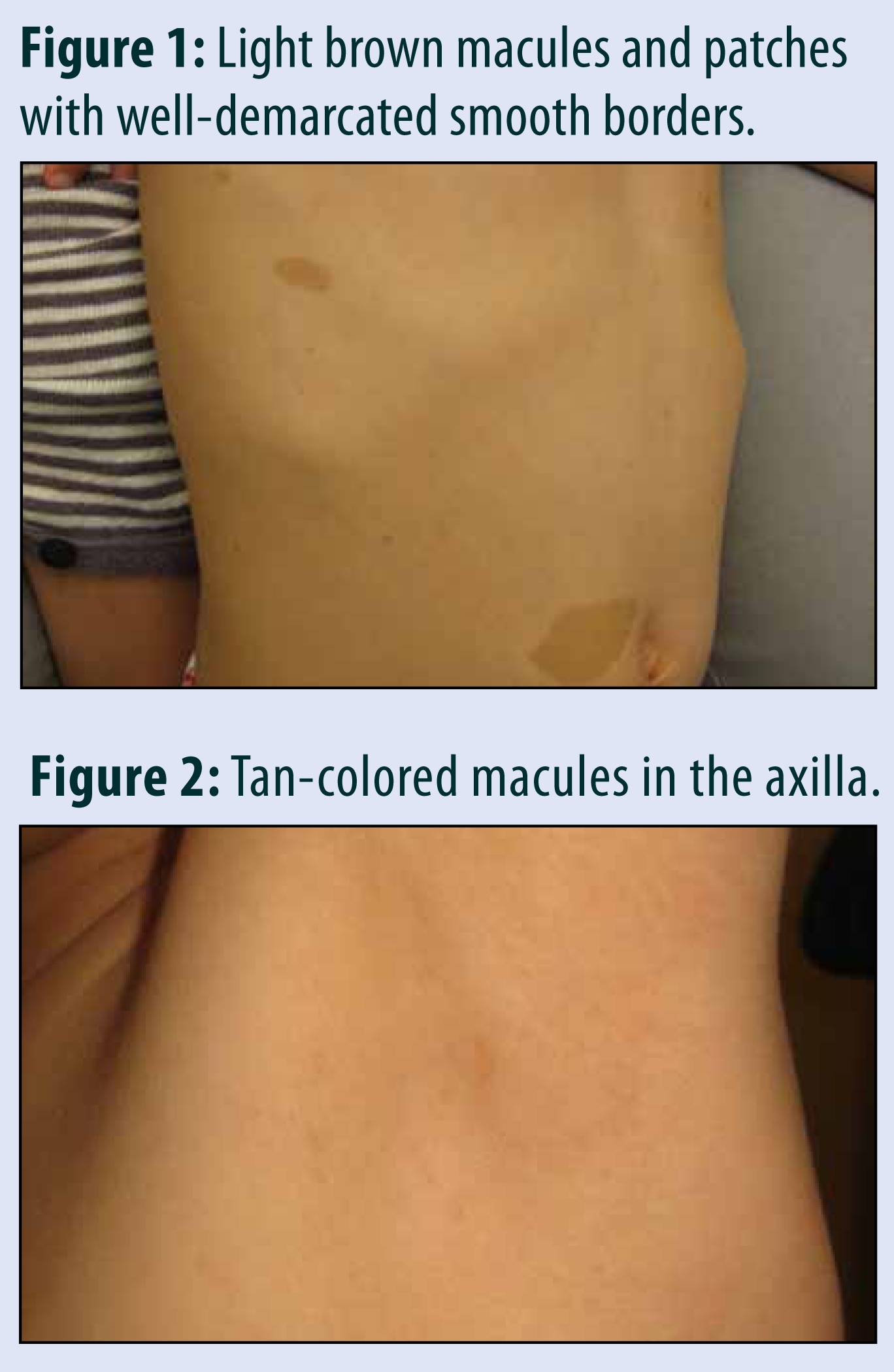
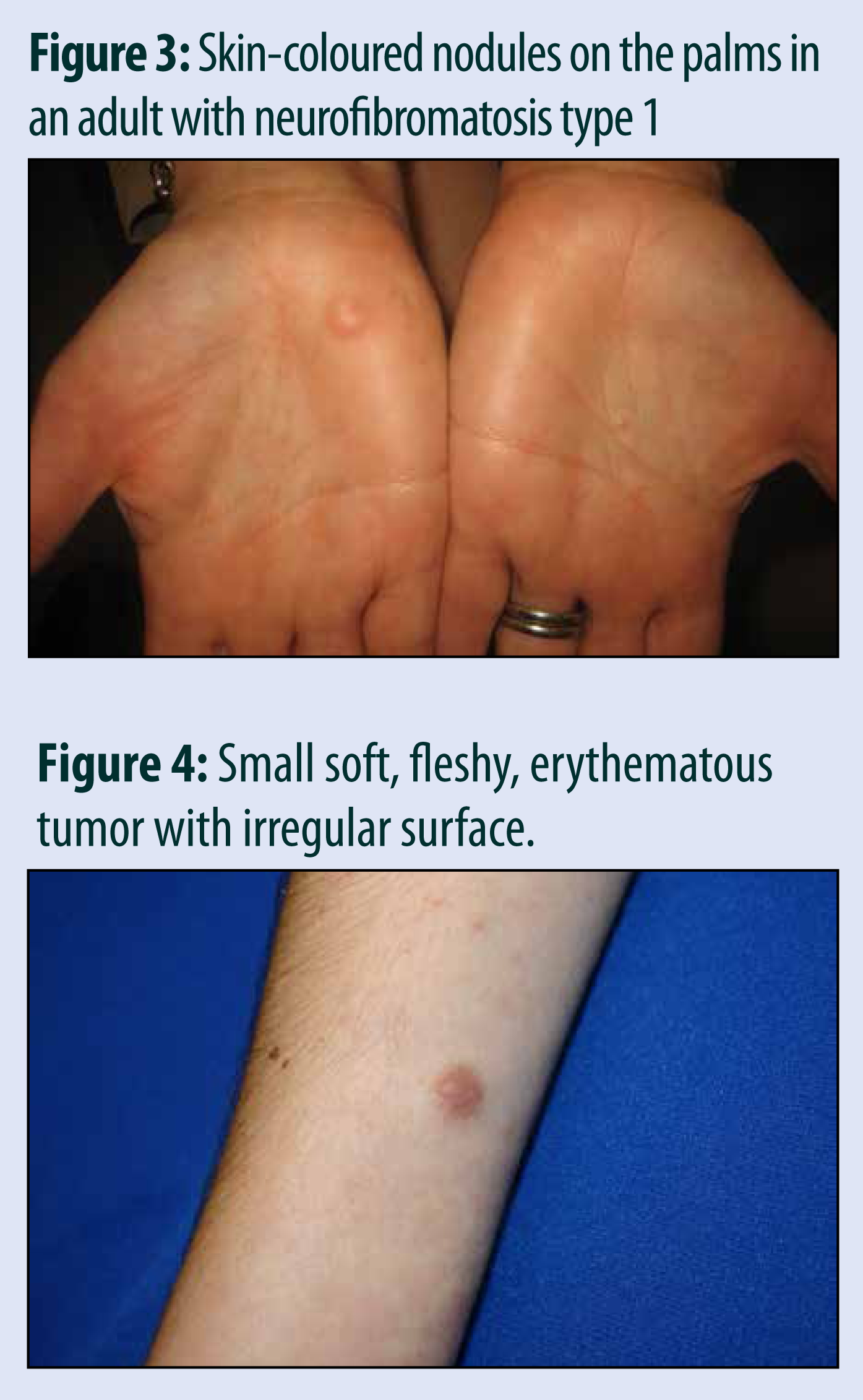
Cutaneous Features of Neurofibromatosis
Cutaneous Features of Neurofibromatosis


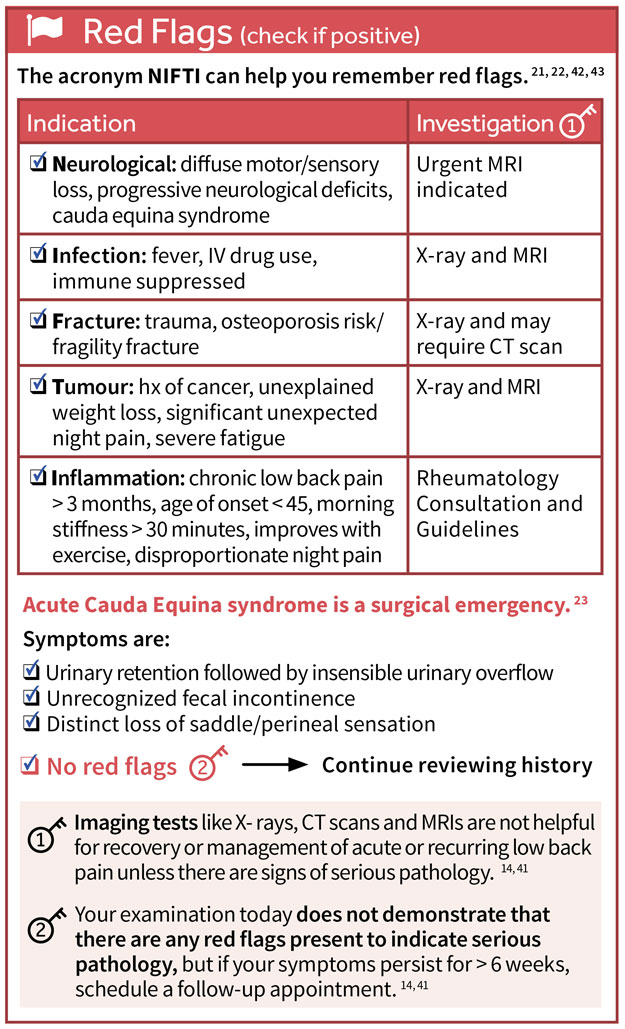
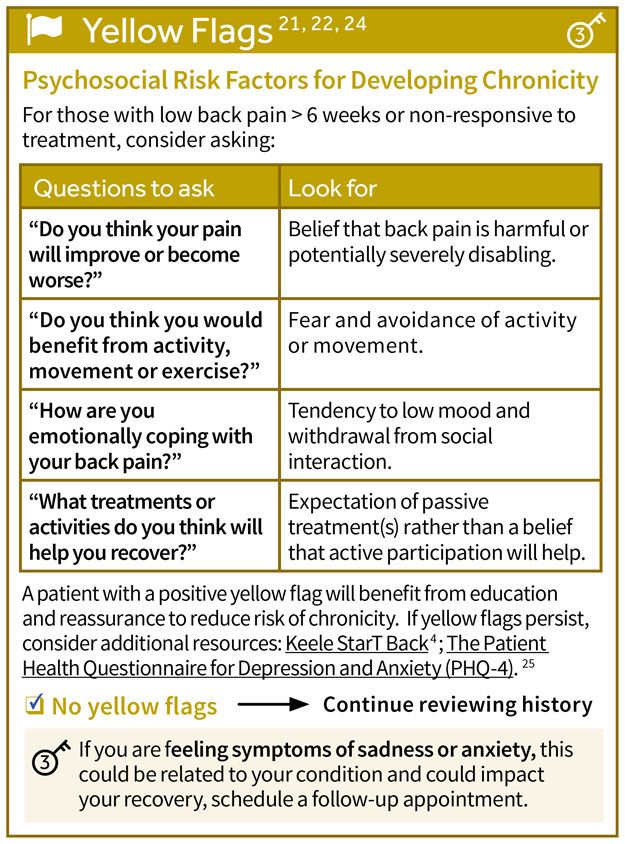
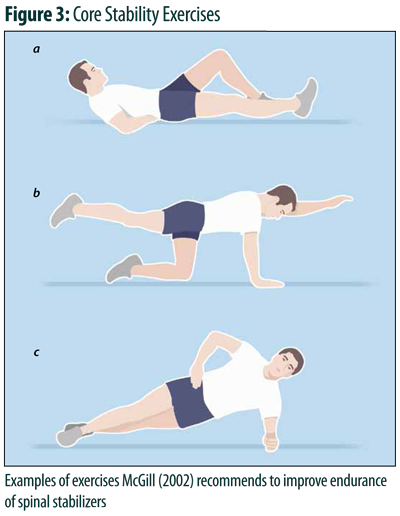
CORE BACK TOOL 2016: New and Improved!
Members of the College of Family Physicians of Canada may claim one non-certified credit per hour for this non-certified educational program.
Mainpro+® Overview