About Rosacea
About Rosacea
WHAT IS ROSACEA?
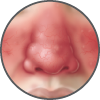
Rosacea is a common, chronic skin condition that causes redness of the face. It often presents as a mild redness or blushing that, over time, lasts for longer durations and becomes more pronounced. Rosacea can also produce enlarged, visible blood vessels and small red bumps on the facial skin. Before diagnosis, it can be mistaken for acne, an allergic reaction, or other skin conditions.1,2,3
- Read more about About Rosacea
- Log in or register to post comments