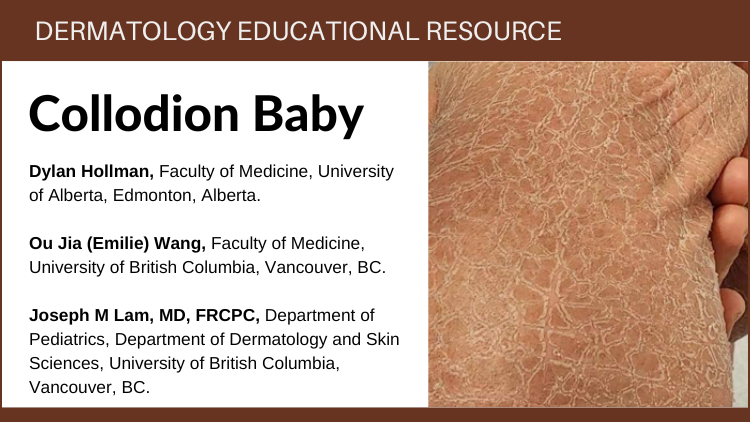
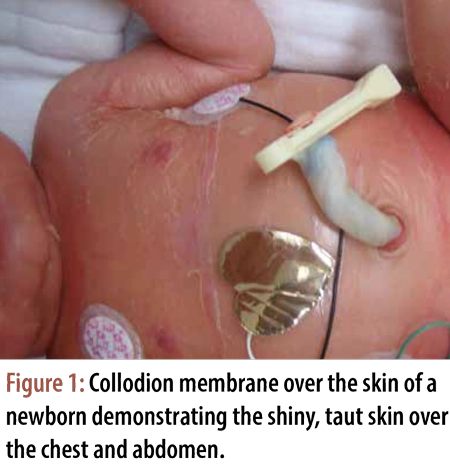
Collodion Baby
Disclaimer:
Disclaimer at the end of each page
Psoriasis is a common but chronic skin condition that causes
inflammation and scaling (red elevated patches and flaking silvery
scales). The patches can be itchy or sore, causing discomfort and pain.
Psoriasis causes skin cells to rise to the surface and shed at a very
rapid rate. On average, people with psoriasis shed their skin cells
every 3 to 4 days, while people without the condition have a turnover
rate of about every 30 days.1,2,3,4
Rosacea is a common, chronic skin condition that causes redness of the face. It often presents as a mild redness or blushing that, over time, lasts for longer durations and becomes more pronounced. Rosacea can also produce enlarged, visible blood vessels and small red bumps on the facial skin. Before diagnosis, it can be mistaken for acne, an allergic reaction, or other skin conditions.1,2,3
Psoriasis is a common but chronic skin condition that causes
inflammation and scaling (red elevated patches and flaking silvery
scales). The patches can be itchy or sore, causing discomfort and pain.
Psoriasis causes skin cells to rise to the surface and shed at a very
rapid rate. On average, people with psoriasis shed their skin cells
every 3 to 4 days, while people without the condition have a turnover
rate of about every 30 days.1,2,3,4
 |
Use sunscreen daily with an SPF 30 or higher with broad-spectrum (UVA and UVB) protection. Sunscreen should be labelled: non-oily, fragrance-free, alcohol-free, and meant for sensitive skin.1 |