1Division of Neurosurgery, Department of Clinical Neuroscience, University of Calgary, Calgary, Alberta, Canada. 2Division of Neurosurgery, Department of Clinical Neuroscience, University of Calgary, Calgary, Alberta, Canada.
Abstract: Osteoporotic vertebral compression fractures (VCFs) are the most common fragility fracture and have significant impact on numerous indices of health quality. High risks patients should be identified and appropriate preventative therapy initiated. The majority of VCFs can be managed in a non-operative fashion, with analgesia as required to support progressive mobilization. Patients who fail non-operative measures may be considered for percutaneous vertebral augmentation. However, the efficacy of these procedures in altering the natural history of recovery is controversial. Surgery has a limited role in the initial management of VCFs and is typically restricted to the rare circumstance of VCF associated with acute neurological dysfunction.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
1. Osteoporosis is under diagnosed in Canada. Early diagnosis, fragility fracture risk stratification and initiation of preventative treatment is important, as osteoporotic vertebral compression fractures (VCFs) have a significant associated personal and societal health utility cost.
2. Patients suspected of having a VCF should have an AP and lateral X-ray of the suspected region. If VCF is confirmed, an upright X-ray should be performed to assess for stability. CT and/or MR imaging has limited utility in the absence of red flag signs or symptoms.
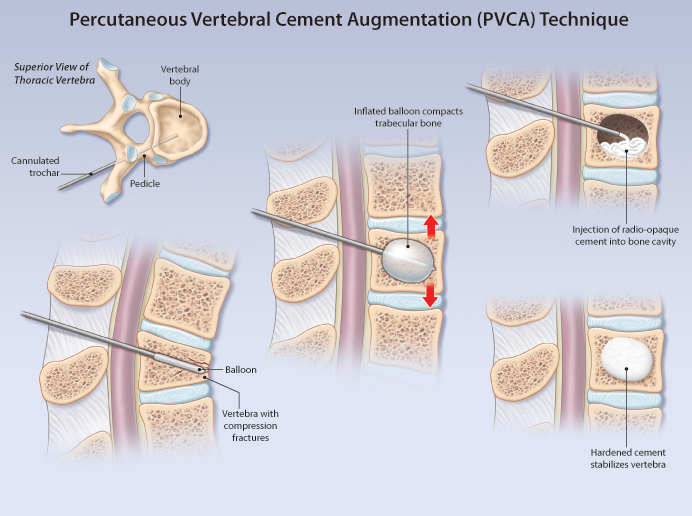
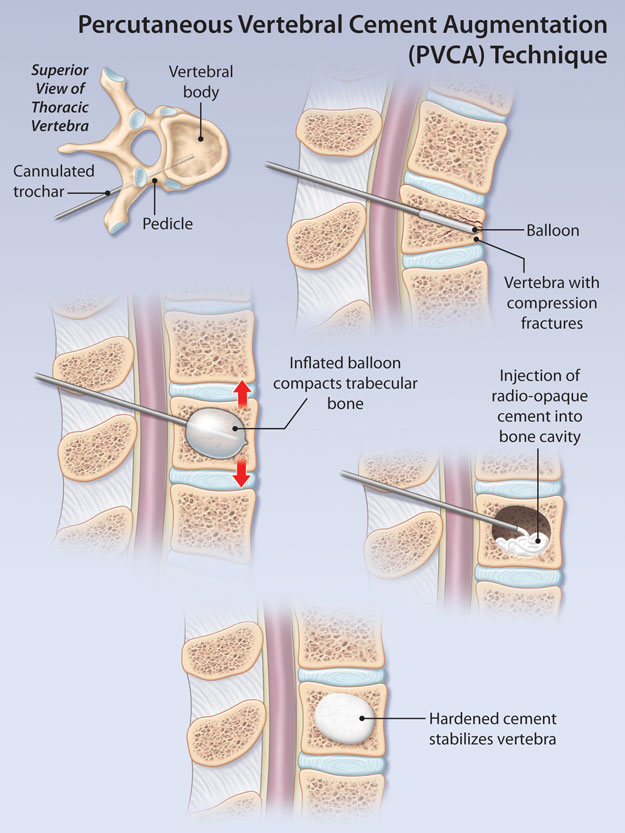
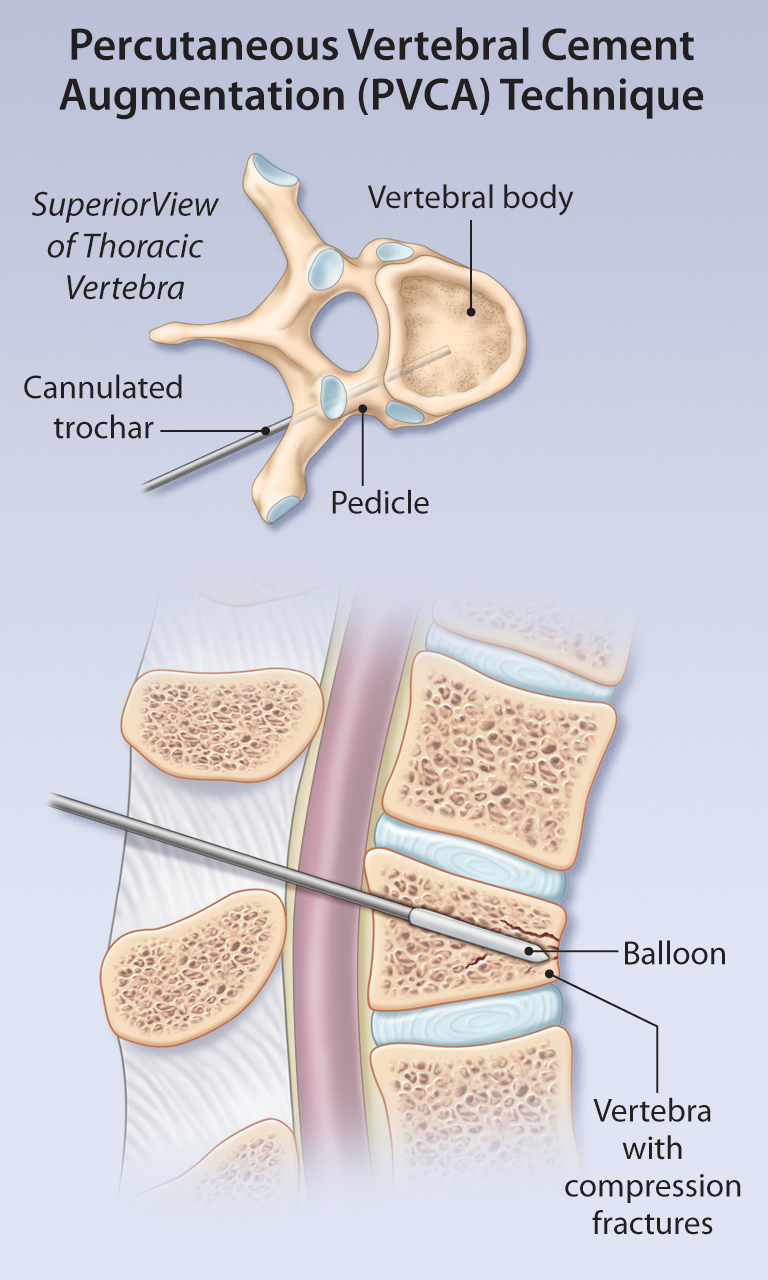
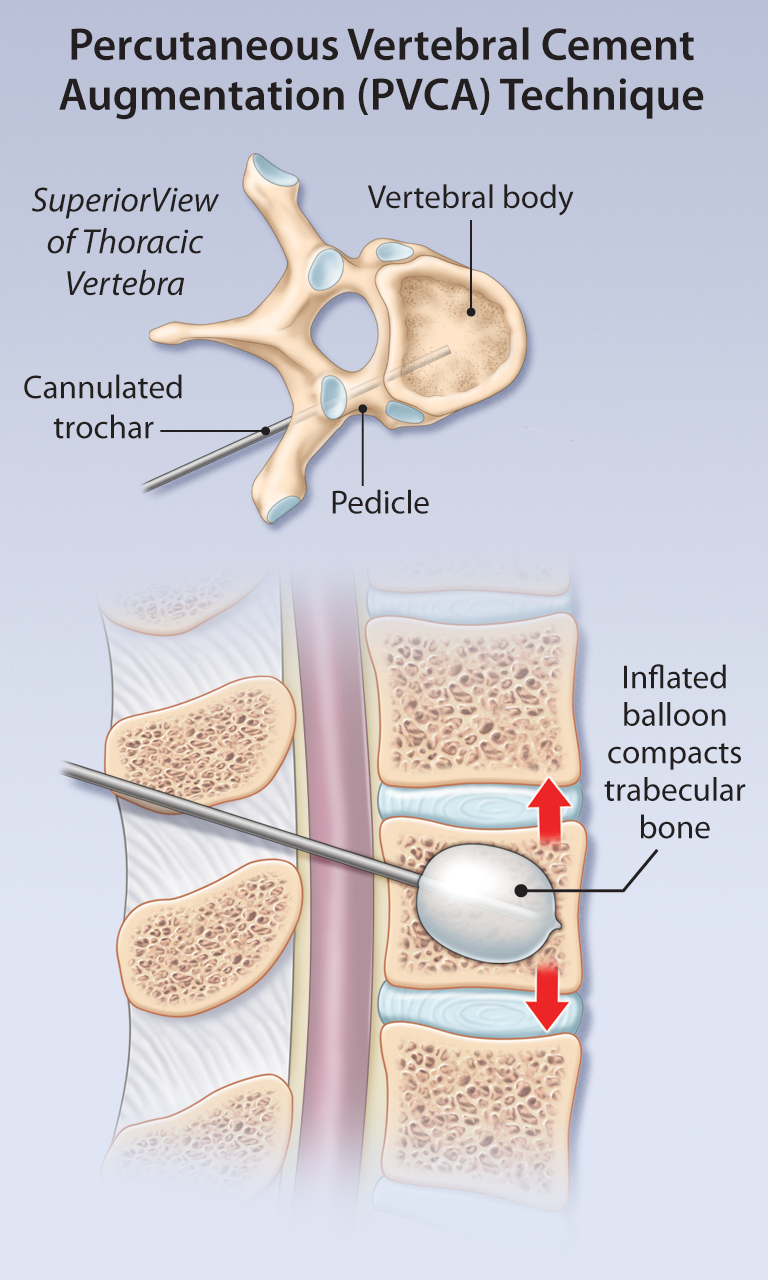
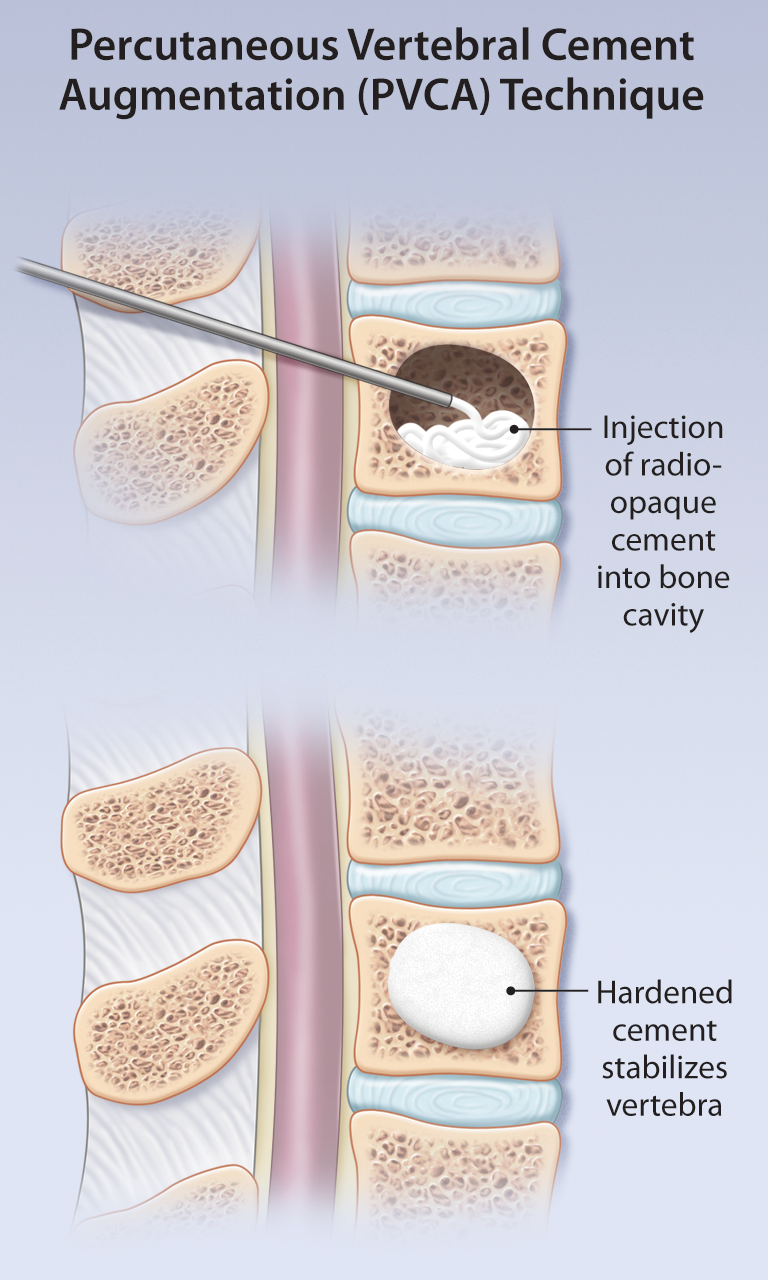
3. VCFs should be managed with initiation of an appropriate pain management regiment, early bed rest as required for pain control and gradual mobilization. Patients with refractory pain 4–6 weeks after onset can be considered for percutaneous vertebral cement augmentation (e.g. vertebroplasty), although the clinical efficacy of such procedures remains unclear.
A few screening measurements can be performed in the office setting to help significantly improve the likelihood of detecting a VCF on radiological studies. They include prospective height loss of greater than 2cm or a height loss, or a height loss based on history of more than 6cm, a rib-to-pelvis distance of less than 2 fingerbreadths, or an occipital-to-wall distance greater than 5cm.
Most patients with osteoporotic VCFs do not need a referral to a spine surgeon. Acute pain from a new VCF usually improves over a period of 6 weeks. Non-operative management should follow the WHO analgesic ladder starting with acetaminophen/NSAIDs followed by opioids, as necessary. The goal of treatment is to provide pain relief and facilitate early functional rehabilitation.
Patients with high or medium 10-year fracture risk should be considered for pharmacotherapy to prevent the progression of low bone mineral density and osteoporotic fractures.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Vertebral Compression Fractures Among Older Adults
Teaser:
Simona Abid, MD, FRCP(C), Geriatric Medicine Fellow, McMaster University, Hamilton, ON. Alexandra Papaioannou, MD, FRCP(C) MSc, Professor, Department of Medicine, Division of Geriatric Medicine, McMaster University, Hamilton, ON.
Vertebral compression fractures (VCF) are the hallmark of osteoporosis, yet two-thirds of all VCF remain undiagnosed and untreated. Both symptomatic and occult VCF are associated with considerable increases in morbidity and mortality, hospitalization rates, admissions to long-term care, and health care-related costs. These fractures increase the risk of future osteoporotic fractures, both vertebral and nonvertebral, independent of bone mineral density. Older adults have lower rates of diagnosis and treatment compared with younger patients, although clinical studies have shown the efficacy and safety of currently available therapies for osteoporosis in older adults are comparable with those in younger individuals. Key words: vertebral compression fractures, osteoporosis, bone mineral density, antiresorptive therapy, anabolic agents.