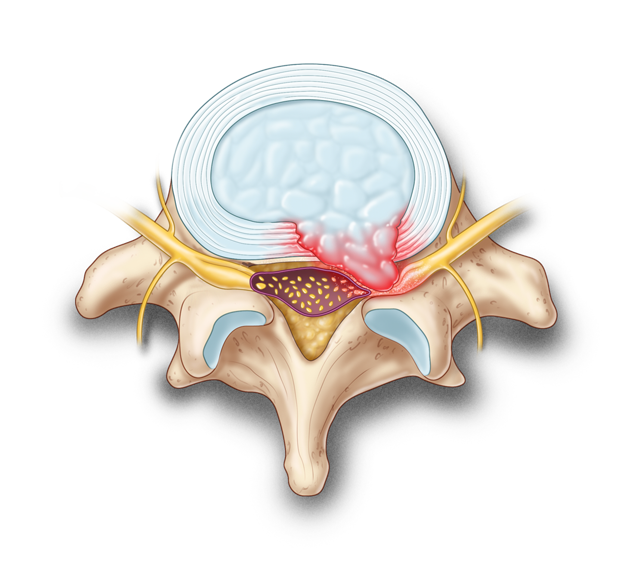
Management of Lumbar Radiculopathy Secondary to Lumbar Intervertebral Disc Herniation
| Questions | 5 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |
| Questions | 3 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |
| Questions | 5 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |
| Questions | 3 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |

Welcome to 3P: pills, pearls, and patients where we will discuss current events in medicine, stories from real patient-physician encounters, and gain insight into what it's like being a physician in today's society.
Back to Pills, Pearls & Patients (3P) Add a Comment
Hello there and welcome to 3P. Pills, Pearls & Patients. I'm your host Dr. Marina Malik.
So welcome. Today is the first episode of Pills, Pearls & Patients. This is the introductory episode where we'll talk a little bit about myself, my practice and what the point of this podcast is and where it's going.
First just a disclaimer. Anything shared on this podcast is obviously not meant to replace any medical advice. It's the opinions of myself and any guests that we might have and if there are any references, they'll always be provided as well.
Please feel free to share any comments that you might have. Obviously we're aiming for an open discussion here and I look forward to you guys interacting with us for this podcast.
So a little bit about myself. As I mentioned, my name is Dr. Marina Malik. I am a fairly new medical graduate in family medicine. I practice in Mississauga, Ontario. I am a Lecturer and Faculty Member of the University of Toronto, Faculty of Family Medicine and Community Medicine. I'm really interested in teaching and medical education and I don't have any particular interests in medicine and I guess that's why i became a family doctor. I like to do it all from young to old, big, small, mental health, respiratory diseases, endocrine diseases, you name it.
I also do have my own personal blog, Health is Wealth and this is where I talk a little bit about my previous experiences as well as just some day-to-day thoughts. So if you're interested in checking it out it's anorexiarecovery1.blogspot.com
 I've also written a book which is called Recipe for Recovery, I battled and Overcame an Eating Disorder and You Can, Too! and that's mostly available on the publisher website at burnstownpublishinghouse.com. Again that's burnstownpublishinghouse.com, and eventually you'll be able to find this podcast transcribed so please feel free to read that afterwards if you're interested in any links as well as any information shared in this podcast.
I've also written a book which is called Recipe for Recovery, I battled and Overcame an Eating Disorder and You Can, Too! and that's mostly available on the publisher website at burnstownpublishinghouse.com. Again that's burnstownpublishinghouse.com, and eventually you'll be able to find this podcast transcribed so please feel free to read that afterwards if you're interested in any links as well as any information shared in this podcast.
So, what's 3P all about? Well, I mean the name kind of says it for itself, Pills, Pearls & Patients. I guess we wouldn't be doctors if we didn't talk about pills, but let's go further into this. Pills is beyond medication, it's more like the medicine that doctors prescribe daily and increasingly these days we're realizing that pills aren't the end-all be-all. Medical treatments these days are procedures, investigations, medications, and a lot of it is really coming down to patient empowerment, as well as collaboration and education. A big portion of managing any illness or any chronic disease these days is definitely allowing the patient to access resources and empowering them to take control and manage their own symptoms. This might be engaging in exercise, adjusting their diet, ensuring that they have good social supports around them, taking part in hobbies, accessing spiritual care, etc. sleep goes a long way too.
What's the Pearls all about in 3P? Pills, Pearls & Patients. Well I guess the aim of this podcast is really talk about some tips, practical advice for physicians all around Canada. I'm interested in sharing real life stories, what really happens with family doctors and doctors in general when they're in practice. What are our emotions and experiences as physicians remembering that physicians are humans too and as much as we'd like to separate work from personal lives it's not always that easy. What are some day-to-day tips that doctors need to know when they're interacting with their patients? Is there any latest evidence or stories that maybe we can share among physicians to help educate our practice and make us better doctors? Another part of the pearls is the highlights of being a doctor. As difficult as being a doctor is, there's a lot of fun to it. I can only imagine how many wonderful stories we might have if we really highlighted the amazing experiences that we have with our patients, albeit there are some really hard days where we're all tired, but there are also some days where you just find that spark again and you sigh and say yes this is why I entered family medicine. I'm sure all of you doctors listening can relate even if it's just that one patient who smiles on their way out or the patient who thanks you when you feel like you've done almost nothing, but yet they're ever so grateful or the day that you put your hands on a belly and think oh that's definitely cholecystitis. You order an ultrasound and there it is in black and white, suspect acute cholecystitis and you are so thankful that you listened to that medical lecture and that you paid attention in your clinical skills when you were examining patients. There are so many pearls to being a family physician and a doctor in general and I hope that this podcast also highlights some of those.
And finally the last P, Patients. Self-explanatory, we wouldn't be doctors without our patients. Sometimes patient encounters can be difficult. There's so many difficult situations that I've seen and I'm sure you can all relate. There's the patients that don't always take their medications or that are late for their appointments or even worse never show up for their appointments. There are the patients who you are just so frustrated about because you want so desperately to help them, but you're not making any leeway or there are the frustrating really sad cases where you've tried everything and so has the patient and yet the prognosis is still poor and it's ever so heartbreaking. Of course there's difficult scenarios as well. Situations like college complaints, feeling like you and the patient aren't seeing eye to eye and not knowing what to do. Those are the really difficult times and this podcast we're going to share some of those difficult times whether it's to open our stories, increase awareness, or even just to support one another.
But there are also lots of happy encounters with patients. As I mentioned before, the joy of feeling like you correctly diagnosed a patient or seeing a patient's eyes light up when they've managed to lower their A1C at their next diabetes visit. Feeling like they've accomplished something or sharing with you as their doctor that they've just gotten the job offer that they were waiting for. As physicians we're so incredibly blessed to have access to so many parts of patients lives that not many people have a window to. In my own experience as a family doctor I truly feel that patients are comfortable sharing a lot of information with me. I actually take lots of delight in listening to patient stories whether it's about you know their job, their time at work, their hobbies. This helps me as a family doctor feel like I've established that therapeutic relationship with my patient and helps me understand a little bit more about them. I no longer see the patient as just a diagnosis or an illness. I've actually gained a complete picture of who they are, what they like to do, who's in their life, what resources they have, and this really helps me take pleasure in my job.
And there you have it in a nutshell. That's the simple explanation of what 3P is about, Pills, Pearls & Patients. As you can see, the aim of this podcast is not meant to focus on just one specific topic in medicine, one diagnosis, one approach to managing an illness, or patient. It's also not meant to be a time where we just rave on and on and on about how great it is to be a family doctor because like i said we have to be honest. Although I love my job and I take so much pleasure in it there's a lot of days where I'm actually tired and on the edge of being burned out and that's why we have to talk about these stories. We have to talk about the Pills, the Pearls, & the Patients.
This podcast is going to be released on a bi-weekly basis and I really encourage and welcome you to listen to every episode, between 20 to 30 minutes long, shouldn't be too long of a time, but I guarantee that you will pick up at least one pearl, no pun intended, during the podcast that will either make you as a physician feel like you're supported, understood, or heard, will make you think about your current practices whether you can relate to some of the stories or tips that we share and who knows might even spark you to share a comment with us about what I should talk about next. I really hope that you'll join me on this journey, bi-weekly.
As an introduction today, I really just want to highlight why Pills, Pearls & Patients was created. I want to reach out and thank the people at Health Plexus and Lumensify for all their support in making this podcast available. Really, Pills Pearls & Patients, 3P, it's about sharing stories, it's about opening up the floor and talking about things that sometimes are brushed under the carpet in medicine. Sharing stories about what patients and physicians go through is incredibly important. There are a lot of patient stories out there. I guess there are a lot of doctor stories out there too, but sometimes I feel like we don't really hear the doctor stories as much. I was speaking to a colleague the other day and we were explaining to one another how sometimes we really want to help our patients, but sometimes we really feel like we're under attack. Sometimes we feel like we just don't know how to help a patient in the best way or for some reason or one another we're misunderstood. This is really difficult and taxing as a family doctor. Most of us, hopefully all of us, have really good intentions, but for some reason when we don't see eye to eye with a patient, emotions might get expressed in maybe not so much of a positive way. I've seen and heard time and time again how family doctors feel like patients might be verbally aggressive towards them. They might feel like patients are attacking them with what they're saying with their experiences and this is really difficult. It feels difficult as a family doctor to want to help people in front of you, but feel like you're not making grounds with them. We hear so often that patients make complaints to the college of family physicians and a colleague of mine was telling me the other day what if doctors were allowed to make "complaints" about patients. I mean it sounds like a funny concept, but think about it, when doctors are "under attack" who do we go to? The police? Not always reasonable. Who do we tell? Mind you we've made several grounds with this, there's a lot out there that's available to help physicians. There's wellness lines the Ontario Medical Association, the CMPA. We've definitely done a lot of work, but there's still a lot of work to be done.
Sharing stories is important to empower physicians. It's important that any family doctor and doctors in general feel like they're not alone and I'm telling you, you are most definitely not alone as much as we all love our job there's a lot of days where we're tired, and as much as there's a lot of days where we're tired, there are so many days where I look and I say wow I would never give up family medicine for even a day in another job.
Talking about our stories and our experiences doesn't always just have to be about the difficult ones between patients and rounds and paperwork and checking lab results, you get the idea. Talking about our stories could even mean what's the latest going on in the news. I would be completely naive not to mention this little thing called the COVID pandemic. Evidence is changing rapidly. Tune in for the next episode where we'll talk about a brief primer on Paxlovid the treatment for COVID. That's now been dubbed as well I guess one of the most evidence-based treatments that we have.
We also should probably talk about the impact of the pandemic not just on ourselves as patients and physicians, but on society in general. There's definitely a role for everyone to play and I think there's a lot of questions that go unsaid. But aside from the pandemic, there's still a lot going on. Today evidence in medicine is changing rapidly. Do you remember back in the day when you would read a medical textbook or god forbid have to go to a library to do a research project on science. Now the internet is widely available and has that many resources fall into our hands. I guess this can be a good thing because now all you need to do is a quick google search and figure out how to convert a GFR into some other random thing. How to calculate a Framingham risk. You can access many apps for your practice as well. Of course there's also the downside to this which is probably a whole other episode, but when patients use Dr. Google sometimes I'm just shaking my head and i know all of you doctors out there can agree about the time the patient read that they should be sticking who knows what in god knows where in order to help themselves feel better. There's so many stories that we should share about this what to not do and what to tell your patients to absolutely avoid.
Talking about stories in medical practice also helps us know what are the resources that we can use. There's so much out there and I myself have learned an incredible amount of things like apps and websites that I can refer my patients to for extra help and support with their condition. On this podcast we'll be sharing some of those things in several episodes, that way as a doctor you can feel like you're making the most of your practice, using your time more efficiently, and when a patient comes to you and says I don't know what to do for this, you might be able to say, hey do you have an iPhone? do you have an Android? and you can share with them some useful apps that they actually might be able to use. We'll also be talking about some resources online because everyone's online and hopefully this will make your practice a little bit more efficient. It'll also help you empower your patients and have something to give them at the end of the visit.
We'll also be having some guest speakers which I think really increases the amount of knowledge and information that we'll be able to share. And certainly if anyone has any other ideas please share with me.
Sharing our stories on this podcast also helps us think about where we are and where we can move forward. No I'm not talking about writing letters to our MPP because to be honest as great as that sounds, I don't have time for that. Between checking my results and making sure I have my hair brushed for work every day, plus putting food on the table, not about to write a letter to my MPP to be honest. Although by all means, if any of you out there have the time I encourage you to get active in society. This is how we make sustainable change and that's another goal for Pills, Pearls & Patients. I hope that by sharing our stories we can think about what do we need to do as a society, as a strong group of empowered and smart and successful physicians, what can we do to change policy, and hear me out on this one change is underneath our fingers. Together we form a strong collaborative group of professionals who can bring about sustainable change, but change starts with us. It starts with sharing our stories, it starts with getting the word out there that something isn't okay in the way we're practicing medicine. In the way we're treating physicians, in the way policy helps or actually doesn't help us help our patients. And then we go about to eliciting this change to making our stories heard, to striving and working together as a community of professionals in collaboration with other healthcare providers, with politicians, with patients, to bring awareness and to make these changes. Change is happening and it's going to continue happening. Opening our voices and opening our hearts to these stories whether they're happy stories, or difficult stories enables us and allows us to bring about these changes.
On that note, I'm going to end with one final thing, which is each person has different stories. Every physician listening to this podcast will definitely have a different experience than my own or with any guest speakers that come. Some of them might be relatable, some of them might not be. Feel free to take whatever is useful and relatable to you and to contemplate and think about what sounds different. Something that I've learned in my time on earth is acceptance and tolerance are very different things. I'm not necessarily asking you to accept everything that's shared on this podcast. Accept means yeah, you listen to it, and you agree with it. I'm asking to promote a spirit of tolerance, tolerance means you and I might have our differences, but we'll listen to one another, we'll be open to the different experiences that are shared on this podcast. We'll be willing to give and take with conversation so that we can learn from one another, so that we can put our hands together as physicians bring about changes open discussions about difficult topics, learn from one another about the latest evidence, and survive as family doctors because let's be honest, being a family doctor is tough, but it's also pretty great. And with that I'm going to wrap up this first episode of Pills, Pearls & Patients or 3P.
I hope you've enjoyed kind of an introduction of what this podcast is going to be about and I am super excited to get talking next episode about Paxlovid and who knows what's happening after that. Well I guess you'll have to stay tuned every two weeks. Thank you so much for being my guest on Pills, Pearls & Patients and I look forward to talking with you in two weeks. Cheers.
Dr. Marina Malak is a family physician in Mississauga, Ontario and a lecturer and faculty member at the University of Toronto. She is actively involved in medical advocacy, and is a board member of the Mississauga Primary Care Network. She is also a member of the National Committee of Continuing Professional Development at the College of Family Physicians of Ontario, and a member of the Research Ethics Board at Trillium Health Partners.
She is passionate about patient care; medical education; and promoting mental, physical, and emotional wellness. She enjoys reading, writing, public speaking, puzzles, doodling in her bullet journal, and creating drawings on Procreate.
| Questions | 5 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |