Abstract:Due to the distinctive anatomic and biomechanical features of the growing paediatric spine, children are susceptible to unique patterns of spinal injuries. Although clinical examination can help guide management, physicians are often required to rely on advanced imaging. Imaging interpretation can be challenging when considering that abnormal parameters among adults, are often within normal physiological limits in children. In general, spinal injuries in children younger than nine years of age are often managed non-operatively, while adolescents are typically managed by adult treatment principles. With the exception of neurologic injuries, most paediatric spinal injuries demonstrate good to excellent prognosis and outcomes.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
Due to the unique properties of the growing spine, including greater elasticity, osseous plasticity, presence of growth centers, relatively strong ligaments, and greater joint mobility, paediatric patients are susceptible to unique fracture patterns and injuries.
There are absolute contraindications regarding return to play decisions.
Children under 13 years of age with vertebral body compression fractures can progressively restore their vertebral height until skeletal maturity.
The vast majority of spine injuries among children under nine years of age, even when relatively unstable, can be managed non-operatively.
Pre-adolescent patients with complete spinal cord injuries are at high risk for developing progressive scoliosis and have not been shown to demonstrate any better neurological outcomes when compared to adults.
The cervical spine is the commonest area of spine injuries with the C1-3 vertebral levels being more commonly seen in children under eight years of age.
A standard immobilization board should not be used for children under eight years of age without an occipital recess or 2-3cm of padding to elevate their body relatively to their head.
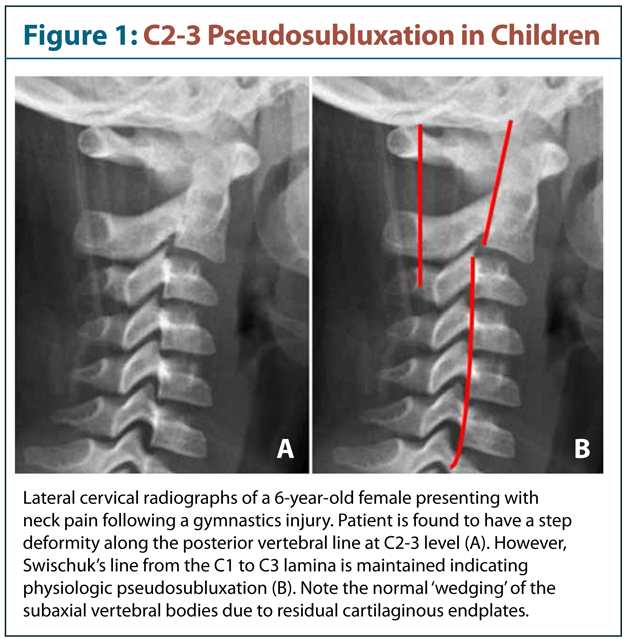
Adult radiographic spinal parameters are often unreliable in children and severe neurologic injuries can be sustained in spite of normal imaging results.
Clinical examination is fairly unreliable for identifying spinal column injuries among pre-school patients and it is often necessary to rely on advanced imaging.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Abstract: Obstructive sleep apnea (OSA) is a disorder in which patients stop breathing repeatedly during sleep, and it is linked to a number of serious medical consequences. However, most patients with OSA remain undiagnosed. The consequences of OSA are particularly severe in children. Adenotonsillar hypertrophy (AT) is a major factor in the etiology of Obstructive Sleep Apnea (OSA) in children. Physicians should consider snoring, pauses in breathing while asleep, restless sleep, bizarre sleeping positions, paradoxical chest movements, cyanosis, bedwetting, hyperactivity, and disruptive behaviour in school as possible indications of untreated OSA in children. The presentation of OSA in children differs substantially from that in adults. For example, hyperactivity is often a primary symptom in children but is not a symptom typically found in adults.
The presentation of OSA in children is significantly different than that in adults; hyperactivity can be a primary symptom in children but is not typically found in adults.
Adenotonsillar hypertrophy is an indicator of undiagnosed OSA in children and merits a sleep study.
Untreated OSA in children can lead to medical and psychiatric issues.
Adenotonsillectomy, a common treatment for OSA in children with large tonsils, not only reduces or eliminates the OSA, but in most cases improves the associated behavioral problems.
Evidence-based medicine supports the need for children with adenotonsillar hypertrophy to be referred to a sleep specialist to be screened for OSA regardless of the degree of tonsillar enlargement.
The I'm Sleepy questionnaire allows doctors to quickly and easily identify children with a high risk of having OSA.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.