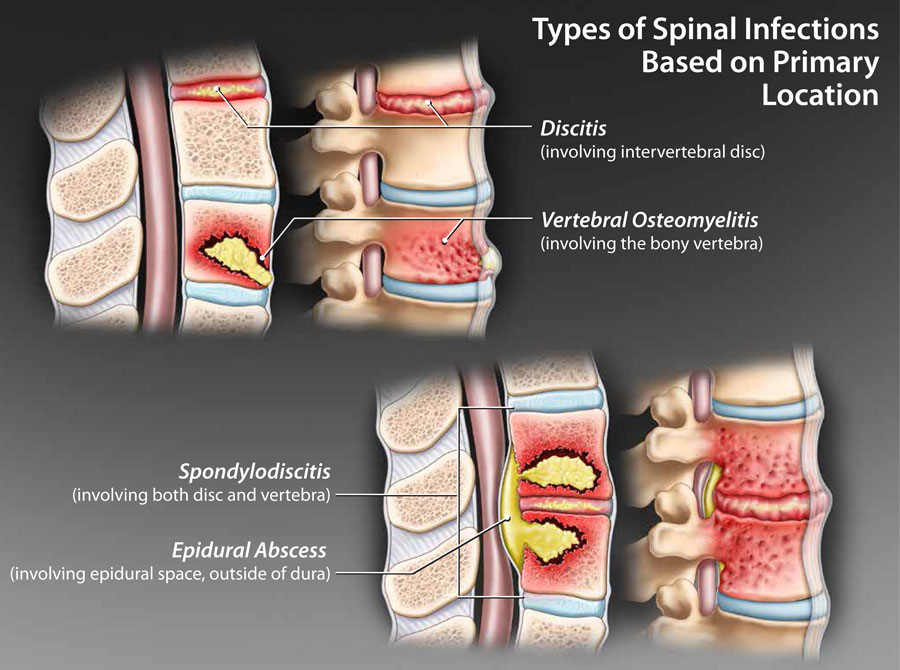
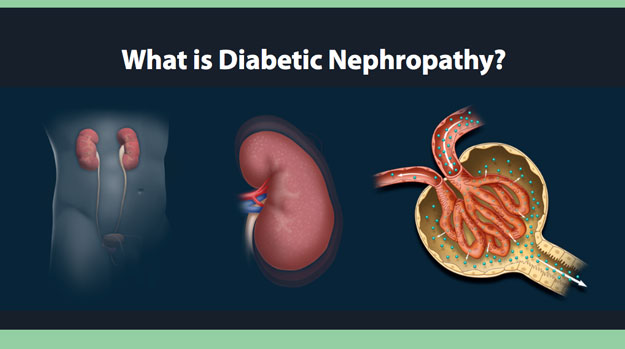
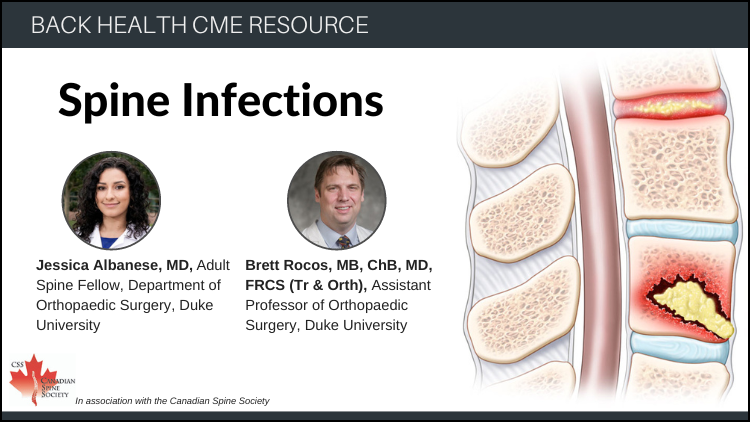
Spine Infections
| Questions | 7 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |
| Questions | 5 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Forbidden |
Dr. Michael Gordon recently retired after a fulfilling career as a geriatrician that spanned 56 years, 44 of which he spent working at the Baycrest Center in Toronto. He is Emeritus Professor of Medicine at the University of Toronto. Dr. Gordon is a recognized ethicist and a thought leader on all topics of care of the elderly and end-of-life decisions. Currently, Dr. Gordon provides part-time professional medical consulting mainly in the domain of cognition and memory loss.