Tichenoff, A.1,2 Holmes, J.D.1,3 Klapak, H.2 Lemmon, J.2 Picanco, M.2 Torrieri, A.2 and Johnson, A.M.1,2
1Health and Rehabilitation Sciences, The University of Western Ontario, London, ON, Canada. 2School of Health Studies, The University of Western Ontario, London, ON, Canada. 3School of Occupational Therapy, The University of Western Ontario, London, ON, Canada.
Abstract
Progressive Supranuclear Palsy (PSP) is a fatal neurodegenerative disorder that is characterized by gaze palsy, bradykinesia, postural instability, and mild dementia. PSP is one of the most common parkinsonian disorders, second only to Parkinson's disease. Of primary concern to individuals with PSP are issues related to reduced mobility, particularly with regards to their increased frequency of falling backwards. Although medical treatment (predominantly pharmaceutical) has been found to be effective for improving some symptoms including slowness and rigidity, most of these interventions are only partially effective in maintaining and improving balance and gait. Mobility issues in PSP are, therefore, addressed primarily through fall prevention programs delivered by physical and occupational therapists. In this review article, we will provide an overview of the current literature that explores nonpharmacological methods for reducing fall risk among individuals living with PSP.
Key words: progressive supranuclear palsy, falls prevention, gait, balance, gait training, balance training, adaptive equipment.
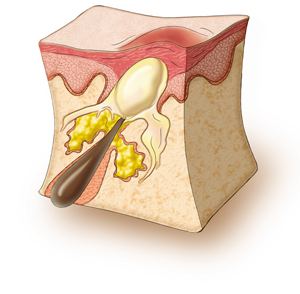 Human skin is covered in hundreds of thousands of microscopic hair follicles, called pores. These are particularly prominent on the face, neck, back, and chest. These pores are connected to oil glands under the skin that make a substance called sebum. Sometimes these follicles produce too many cells and become blocked. As a result, sebum (oil) gets trapped and bacteria (P. acnes) begin to grow.1,2,4
Human skin is covered in hundreds of thousands of microscopic hair follicles, called pores. These are particularly prominent on the face, neck, back, and chest. These pores are connected to oil glands under the skin that make a substance called sebum. Sometimes these follicles produce too many cells and become blocked. As a result, sebum (oil) gets trapped and bacteria (P. acnes) begin to grow.1,2,4 Treatment for acne has several goals: to heal pimples, to prevent pimples (by decreasing sebum production, killing bacteria, and normalizing skin shedding), and to prevent scarring.1,6
Treatment for acne has several goals: to heal pimples, to prevent pimples (by decreasing sebum production, killing bacteria, and normalizing skin shedding), and to prevent scarring.1,6 Michael Gordon, MD, MSc, FRCPC, Medical Program Director, Palliative Care, Baycrest Geriatric Health Care System, Professor of Medicine, University of Toronto, Toronto, ON.
Michael Gordon, MD, MSc, FRCPC, Medical Program Director, Palliative Care, Baycrest Geriatric Health Care System, Professor of Medicine, University of Toronto, Toronto, ON.
 Are the symptoms permanent?
Are the symptoms permanent?