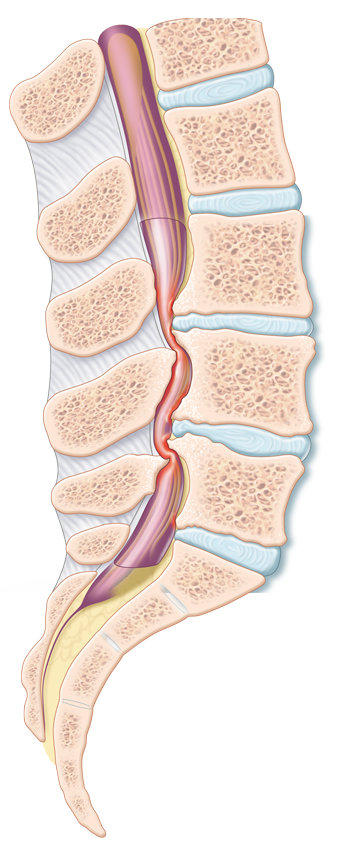
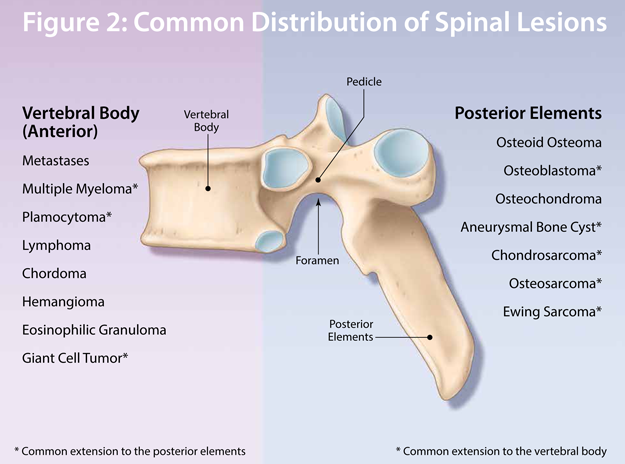
Spinal Lesion: Benign or Malignant? When should you worry?

Disclaimer:
Disclaimer at the end of each page
| Questions | 5 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |
| Questions | 3 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |

When caring for older adults with comorbidities, especially those at the extreme upper limits of life, it may be easy for providers to lessen the intensity of their curiosity and medical investigation. For some older individuals’ chronic conditions, the odds of a positive outcome may seem too distant or the patient’s discomfort—or, in many jurisdictions, the financial burden—may act as a barrier to the pursuit of answers.
Sometimes it can seem like the answer itself is unlikely to result in any meaningful benefit to the patient. When providers see an older patient with what appears to be a chronic condition, who is physically and mentally declining, it is not unusual for the provider to just accept it as a natural consequence of extreme aging. Patients themselves and their families are willing to accept futility as well, even if reluctantly, when the “verdict” comes from a physician—especially if it is a “specialist.”
One such example of this kind of case—what might be called “beneficent ageism”—occurred in my ambulatory geriatric practice. The patient was 95 years old when I first encountered her in my office accompanied by two devoted daughters who were committed to her care and fixated on the task of trying to allow her to live out most of her life in the communal home (one daughter lived with her with her family and the other lived close by). They were truly doting children.
The patient’s main complaint was cognitive impairment, and she fit the usual criteria for mild dementia with a range of vascular risk factors—she actually was started on and responded modestly to donepezil. With this positive result, it became clear that she had other bothersome symptoms that had, over time, been attributed to her age. For example, she became easily short of breath and had been to emergency rooms (ERs) over the years with what had been construed as heart failure due to a mixture of hypertension with (what seemed to be) mild chronic lung disease of uncertain etiology. She was maintained on the usual collection of vascular enhancers and pulmonary puffers, which afforded her some comfort with the acute episodes that had resulted in ER visits—an extra dose of furosemide and some intensive bronchodilator therapy.
She also had modest anemia, which had never really been looked into and seemed merely incidental. It was treated intermittently with blood transfusion for which no clear etiology was found—she had normal blood levels of B12, folate, and iron but a moderately low ferritin for which iron had been given with minimal benefit to her hematological parameters.
At the age of 97, I consulted with her attending physician and specialists to see what the cause of her anemia was and whether it could be possible that the degree of anemia might be compromising not only to her cognitive function but to her cardio-respiratory function. The daughters agreed that after blood transfusion she always seemed better in terms of her cognition and “breathing,” whereas, when the levels began to fall, she would often be short of breath at rest with little in the way of exercise reserve. Despite a number of enquiries, I could not convince any of the other physician specialists to agree to have her referred to a hematologist. Having heard about the possibility of a bone marrow biopsy with a hematologist, the daughters were even reluctant to intervene with an investigation that might cause her discomfort. I explained the procedure (having had a few myself for personal medical problems) and said, if by chance something were found, it might respond to medication that could stimulate the blood-making process of the body. The hematologist referral was eventually accepted with reluctance by the patient and her daughters.
One day a fax came through with a letter from a nephrologist and the hematologist indicating that they would forego an actual bone marrow evaluation to avoid discomfort but felt that the patient’s minor renal impairment combined with her other chronic disease burden might respond to therapy with erythropoietin.
About 8 weeks later, the patient and her daughters came into my clinic, early for the appointment as usual. When I saw them in the waiting area, they waved at me, and I could not help but note that the patient was not huffing and puffing as I had previously seen her—even while sitting. When their turn came and I could see her close-up, I saw that her skin color was more robust than usual, that she indeed was not huffing as she spoke to me, her cognition was at least as good as previously, and, if anything, the content of her speech and language appeared better. The more communicative daughter handed me a sheet of paper on which numbers were written. “You would not have received these yet as they are only from yesterday, so I copied them down for you—unbelievable.”
Indeed the numbers were impressive with a hemoglobin level that had gone up almost 20 points from the previous 6-month average. Her skin color and conjunctival color was close to normal. But most impressive was her breathing pattern and the animation of her speech. The daughters were beside themselves with glee and the patient thanked me—by name—which she was not always able to do.
There is an adage that goes something like “age alone cannot be used to determine the likelihood of usefulness of treatments.” While it should be understood that age is an important component of decision-making, if the investigation and treatments are not onerous by nature, they should not be discarded simply because of the high-age factor. Indeed, nothing should interfere with a thorough analytical review of possible diagnostic and treatment options for each individual a medical provider encounters.
This article was originally published online at https://www.managedhealthcareconnect.com/blog/abandoning-treatment-due-age-alone

D’Arcy Little, MD, CCFP, FRCPC Medical Director, JCCC and HealthPlexus.NET
For those of us who are planners, it seems perfectly natural to anticipate the possibilities of the future and try to take steps to either avoid bad outcomes or implement steps to mitigate deleterious outcomes. My late father, an engineer whose expertise was motor vehicles, drummed into me the importance of timely oil changes—which I do to this day: it is an almost obsession with me. I constantly have to remind my children to keep up the schedule and over time they are getting better at it as I give them visual images of burned out engines, and the need for early retirement due to expensive maintenance costs of their cars.
For those like me who attend to elders as patients, with the usual accompaniment of their spouses and/or children, beyond clinical care, much of my time and effort focuses on planning for the future. Because my clearly defined domain is medicine, that is always the first level of interaction of clinical relationships. However within a short period of time depending on the length and duration of our relationship I try to focus on future planning—in all domains (what is often called advance care planning) and more recently on documentation of all the necessary information that makes it easier for families to cope with the challenging life events including severe illness or death.
During the past few years I have experienced on a personal level and extended family level the risks, benefits and barriers to planning for the unexpected and although foreseen theoretically always seems to be projected well into the future. One has often heard the phrase "Nothing focuses the mind like a hanging", attributed to the 18th century, poet, writer and critic, Samuel Johnson. Some people deal with the knowledge of a new and potentially debilitating or even eventually fatal illness with disbelief or the quest for an alternative diagnosis or as postulated by the Swiss Psychiatrist Elisabeth Kubler-Ross which in the original form included:
The stages, popularly known by the acronym DABDA, (from Wikipedia July 12, 2017):
What is missing from this time honored construct of the stages of dealing with serious illness or impending death is what plans one undertakes to make sure everything is in place no matter the outcome. Like an impending hanging—one should focus one's mind on the often ordinary and mundane plans to make sure that one's family is not left to struggle with the emotional challenge of loss and have it compounded by incomplete and scattered financial and estate plans without clear direction as to whom one should contact to do what?
Anyone who has been through this process either as the person diagnosed with a serious disease or has witnessed the occurrence in a close family member or friend is likely to recognize the common failures when it comes to proper preparation. One approach that I have found useful when explaining to my patients and their families the importance of such planning is to go through the major steps that are involved, using as plain language as possible. Having a check list guide is another way of making sure that the important issues are addressed and documented.
Although it may seem self-evident, the first step is often dealt with as a crises rather than a well-planned process:
Arranging for the funeral and burial:
I became a convert to the pre-arranged and pre-paid funeral many years ago after I arranged it for myself—as a way of avoiding my family having to deal with such an emotionally fraught process in the time of crises and mourning. I found through the process I went through that the funeral home was very organized, dealt with all the issues and at the end provided me with the necessary documentation and contact numbers so that when necessary one phone call and the account number would assure the process would take place as I had wished it, not under the duress of making decisions such as type and expense of the casket. As an aside, pre-paying results in a financial saving as the payment is in current dollars not an inflated price in the future. If the person in question travels a lot it is worth paying the slight premium for return of the body to one's home town from anywhere in the world which could potentially cost a great deal.
Contacting critical people:
Aside from contacting close family members the critical people I am referring to: One's lawyer; financial advisor(s); insurance agent; bank manager; wills executor and accountant. With the help of this team, most if not all if the issues related to death and the issue of interpretation of the will, procedures around the release and distribution of assets can be undertaken in the most time efficient and non-emotional fashion. One should discuss the important points with the spouse or children who would be survivors to make sure everyone who should be in the loop of decision-making is properly prepared and informed. Arrangements for immediate cash-flow should have been anticipated and arranged so that there is no problem with paying necessary expenses while awaiting the final distribution of assets.
Making necessary documents readily and clearly available:
This is one of the most important steps in the estate planning process, one of the most difficult and tedious and the one which if not done well can leave one's loved one's high and dry or at least spending lots of trying to find important documents. Of the necessary documents that must be found as soon as possible during the latter days of a loved one's illness and after the death of a loved one is:
Practical tips:
Gathering all of the pertinent documents into one binder or file would the usual way of gathering and making available this information. Putting it into an Excel spread sheet would be another way and keeping that file readily available would be more contemporary way of doing it. Using one of the many commercial products available to facilitate a digital record might make the task easier and allow for easy editing and updating and if done properly make it hard to hack or disrupt the record that may be kept in a digital format.
One product among others I am impressed with is LifeBank™. There are a number of apps for IOS and Android and on line portals for keeping a record of medical reports, etc. There are what are called ehealth Wallets—a la Microsoft's HealthVault, Apple Health and Google Fit. There a variety of apps like myPHR, WebMD and Humana. Each suffers from a deficiency in one way or another. Clearly being on line via the cloud exposes all one's medical info to the "world" of hacking—now so widespread and pervasive. Many of the apps are also focused on fitness. Others, like the Humana, concentrate on a record of claims made.
LifeBank™—whose tag is Collect and Protect—can be used as a data key, totally off the cloud, or retained on one's computer or laptop. Either way, it contains a suite of forms providing a complete record from A to Z of all aspects of one's life. One significant and noteworthy feature of LifeBank is that one can scan into it—or via a cut and paste—all manner of documents including all of one's health-related records. Inter-activity with one's hospital or clinician is immediately enhanced! Leaving aside the value and security of being armed with all the information about oneself 24/7 in the event of an emergency, medical or otherwise, one's nearest and dearest—or an appointed trusted person like one's lawyer or accountant—can also be provided with a copy data key (for safe-keeping) or know where to access it should it become necessary. LifeBank is structured as a formatted document which reminds the user of the categories that need to be documented.
Conclusion
End of life planning is difficult enough although once undertaken most people can express their wishes and preferences to their loved ones and those who will be their substitute decision makers. Having the final medical preferences, documents such as the advance directives (living wills) and the estate planned information readily available will make the emotionally difficult task of implementing all the components of an estate plan will help make sure it goes as smoothly as possible.
| Questions | 5 |
|---|---|
| Attempts allowed | Unlimited |
| Available | Always |
| Pass rate | 75 % |
| Backwards navigation | Allowed |