Medical Director, Journal of Current Clinical Care and www.healthplexus.net, Adjunct Clinical Lecturer, Departments of Medical Imaging and Family Medicine, University of Toronto,
Toronto, ON.
Abstract:Background: Effective collaboration between radiologists and ordering physicians is essential for optimal patient care, yet tensions can arise when radiologists suggest alternative imaging approaches. This article examines the importance of evidence-based imaging selection and provides a framework for improved interdisciplinary collaboration. Purpose: To demonstrate how collaborative imaging decisions, particularly in critical diagnoses such as spinal infections, can improve patient outcomes while reducing medicolegal risk, and to offer practical strategies for enhancing communication between radiologists and ordering physicians. Methods: We review current literature comparing imaging modalities for spinal infections, analyze medicolegal implications of imaging choices, and propose institutional and technological solutions for improved collaboration. Results: Evidence demonstrates significant superiority of MRI with intravenous contrast over CT for diagnosing spinal infections, with MRI showing 96-100% sensitivity versus CT’s 66-84% sensitivity for discitis/osteomyelitis. For epidural abscess detection, MRI approaches 100% sensitivity while CT ranges from 50-90%. Missed diagnoses due to suboptimal imaging choices represent a significant source of malpractice litigation. Conclusion: When radiologists suggest alternative imaging approaches, these recommendations represent evidence-based efforts to optimize patient care rather than challenges to clinical autonomy. Successful collaboration requires mutual respect, open communication, and shared commitment to evidence-based practice. Implementation of multidisciplinary conferences, clinical decision support systems, and rapid consultation protocols can significantly improve imaging appropriateness and patient outcomes.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
Collaboration Improves Outcomes—Effective communication between radiologists and ordering physicians enhances diagnostic accuracy and patient care, especially in complex cases like spinal infections.
MRI is Superior for Spinal Infections—MRI with contrast offers significantly higher sensitivity and specificity than CT for diagnosing discitis, osteomyelitis, and epidural abscess, leading to earlier and more accurate detection.
Missed Diagnoses Carry Legal Risk—Inadequate imaging choices can lead to delayed diagnoses and serious complications, increasing the risk of malpractice claims and emphasizing the need for evidence-based imaging.
Practical Strategies Enhance Teamwork—Institutional tools like multidisciplinary conferences, clinical decision support systems, and rapid consultation protocols foster better collaboration and imaging appropriateness.
Always prioritize MRI with contrast for suspected spinal infections—it offers near 100% sensitivity and can detect early changes invisible on CT, enabling timely diagnosis and intervention.
When radiologists suggest alternative imaging, it’s a clinical partnership—not a challenge to autonomy. Their input is grounded in evidence and aimed at optimizing patient outcomes.
Don’t rely solely on negative initial imaging—if clinical suspicion for spinal infection remains high, pursue further evaluation, as early imaging (especially CT) can miss critical findings.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Medical Director, Journal of Current Clinical Care and www.healthplexus.net, Adjunct Clinical Lecturer, Departments of Medical Imaging and Family Medicine, University of Toronto,
Toronto, ON.
Abstract: Ovarian dermoid cysts, or mature cystic teratomas, are the most common benign ovarian neoplasms, typically affecting women of reproductive age. These germ cell tumors contain tissues from multiple layers and present variably, from asymptomatic findings to acute complications like torsion or rupture. Accurate imaging through ultrasound, CT, or MRI is crucial for diagnosis and management, ranging from observation to surgical intervention based on size, symptoms, and malignancy risk.
Ovarian dermoid cysts account for 20-25% of all ovarian tumors, predominantly in women aged 20-40 years.
Common imaging features include fat-fluid levels, calcifications, and the Rokitansky protuberance, which guide diagnosis.
Conservative management is feasible for asymptomatic cysts smaller than 6 cm, while surgical removal is indicated for symptomatic or complex cases.
Advanced imaging techniques like MRI enhance malignancy detection and pre-surgical planning.
Imaging Techniques: Ultrasound often reveals characteristic features such as the “tip of the iceberg” sign and mixed echogenicity, aiding early detection.
Complication Indicators: Acute severe pain with nausea may indicate torsion or rupture, necessitating immediate intervention.
Surgical Preference: Laparoscopic cystectomy is minimally invasive, preferred for preserving ovarian tissue and preventing rupture.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Radiologist, Orillia Soldiers' Memorial Hospital, Adjunct Clinical Lecturer, Department of Family and Community Medicine and Department of Medical Imaging, University of Toronto, Toronto, ON.
Abstract: Prostate cancer is a common cancer in men worldwide, and early detection is key to improved patient outcomes. Diagnosis typically involves a combination of clinical examination, prostate-specific antigen blood testing, and imaging studies. Radiology plays an important role, aiding in treatment planning, confirming the diagnosis by directing biopsy, staging the patient, and following treatment course. Imaging modalities for prostate cancer diagnosis include ultrasound, CT, nuclear medicine, and MRI. While MRI is the most sensitive imaging modality, ultrasound is still the preferred modality for measuring the prostate volume. Prostate-specific membrane antigen PET imaging has shown to have superior sensitivity and specificity compared to conventional imaging modalities in the detection of prostate cancer, especially in the context of low PSA. Clinical pearls include performing ultrasound-guided biopsy under local anesthesia to improve patient comfort, and the use of fusion MRI and ultrasound images to facilitate MRI/TRUS fusion-guided biopsy.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
Radiology plays a crucial role in prostate cancer diagnosis, aiding in treatment planning, confirming the diagnosis, and directing biopsy.
Imaging modalities for prostate cancer diagnosis include ultrasound, CT, nuclear medicine, and MRI.
MRI is the most sensitive conventional imaging modality for detecting prostate cancer.
Prostate-specific membrane antigen PET imaging has been shown to have superior sensitivity and specificity compared to conventional imaging modalities in the detection of prostate cancer, especially in context of low PSA.
Ultrasound is still the preferred modality for measuring the prostate volume.
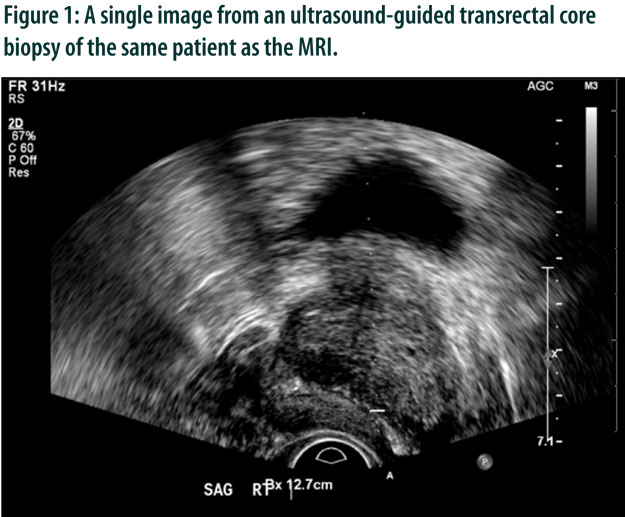
Ultrasound-guided biopsy is a minimally-invasive procedure that involves inserting a needle through the rectum via an ultrasound probe guide and into the prostate gland. It is performed under local anesthesia and patients are discharged the same day after a short period of observation in the radiology department.
MRI and ultrasound images can be fused to facilitate MRI/TRUS fusion-guided biopsy, which improves the accuracy of the biopsy procedure.
The use of antibiotic prophylaxis before ultrasound-guided biopsy decreases the risk of infection to approximately 1 in 100 patients.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.