1Department of Anesthesia, Providence Healthcare, Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Vancouver, BC, Canada. 2Department of Anesthesia, Providence Healthcare, Department of Surgery, University of British Columbia, Vancouver, BC, Canada. 3Department of Surgery, Section of Neurosurgery, University of Manitoba, Health Sciences Centre, Winnipeg, MB, Canada. 4Department of Anesthesia, Providence Healthcare, Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Department of Surgery, University of British Columbia, Vancouver, BC, Canada. 5Department of Anesthesia, Providence Healthcare, Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Department of Surgery, University of British Columbia, Vancouver, BC, Canada.
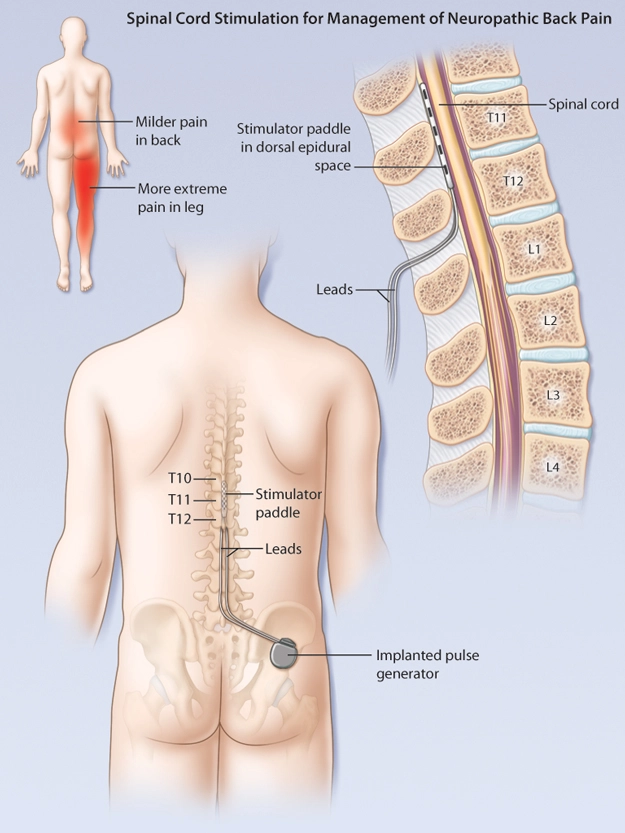
Abstract: Chronic neuropathic pain is associated with substantial disability and societal economic impact. Formerly called Failed Back Surgery Syndrome, and now labelled as Chronic Pain after Spinal Surgery by the ICD-11, this entity represents persistent neuropathic leg pain following structurally corrective spinal surgery, often refractory to pharmacological and interventional management,. In appropriately selected patients where medical management has been unsuccessful, the minimally invasive surgical technique of spinal cord stimulation can reduce disability and pain. Technological advances continue to improve this approach with greater success, lessened morbidity, and expanding indications.
Key Words: chronic pain after spinal surgery, failed back surgery syndrome, neuropathic pain, spinal cord stimulation, neuromodulation.
Members of the College of Family Physicians of Canada may claim MAINPRO-M2 Credits for this unaccredited educational program.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
1. Managing chronic pain after spinal surgery is a challenging and requires combined pharmacological and interventional options.
2. Spinal cord stimulation is a modality with strong evidence to supports its efficacy in the management of patients with chronic pain after spinal surgery.
3. The workup of patients with chronic pain after spinal surgery must include multi-tier pharmacological approaches, psychological optimization, and structural spinal assessment from a multidisciplinary group of clinicians.
Neuropathic pain is defined as pain caused by a lesion or disease of the somatosensory nervous system1. Spontaneous features include burning pain and tightness with unpredictable lancinating features.
The mechanism of spinal cord stimulation involves multiple sites within the central and peripheral nervous system. SCS can influence levels of cerebrospinal fluid neurotransmitters including increases in GABA, serotonin, Substance-P, norepinephrine, acetylcholine, and adenosine, and decreases in glutamate and aspartate.
The differential target multiplexed (paresthesia-free) spinal cord stimulation programs appear superior to the older standard paresthesia-based approach.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
1Faculty of Medicine, University of British Columbia, Vancouver, British Columbia, Canada. 2Department of Pediatrics, University of British Columbia, Vancouver, British Columbia, Canada. 3Department of Pediatrics, Department of Dermatology and Skin Sciences, University of British Columbia, Vancouver, British Columbia, Canada.
Abstract: Urticaria is a common, mast cell-driven disorder that presents with transient wheals, angioedema, or both. Clinically, it is classified into acute or chronic, depending on the duration of symptoms, and further classified by the presence or absence of inducible stimuli. Although urticaria is rarely life-threatening, it can reduce quality of life and carry significant socioeconomic burden on patients. While there is no cure to the disease, the treatment algorithm for urticaria focusses on the control of symptoms with antihistamines as the mainstay of therapy and immunosuppressive/immunomodulating therapies for severe cases.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
Urticaria is a common pruritic condition that is divided into acute or chronic forms. It can be idiopathic or inducible by triggers that including foods, medications, infections, environmental factors, physical stimuli, and medications.
Acute and chronic urticaria are clinical diagnoses guided by a detailed history and physical examination, and diagnostic testing is not routinely indicated, unless clinical suspicion warrants exclusion of underlying causes.
Pathogenesis of urticaria involves mast cells and subsequent release of histamines and proinflammatory mediators that result in sensory nerve activation, vasodilatation, and plasma extravasation with leukocyte recruitment to lesions.
Second-generation, non-sedating H1-antihistamines are the mainstay of treatment for all types of urticaria and dosed up to fourfold to achieve adequate control.
Individual wheals typically resolve within 24 hours without leaving residual changes on the skin. If the duration of wheals is unclear, patients or clinicians can draw a line around the lesion to observe for changes or resolution
In addition to the physical stimuli in chronic inducible urticaria, other triggers of chronic urticaria include psychosocial stress, work exposures, surgical implants, and menses.
Investigations are not needed to make a diagnosis. However, a limited work-up can be considered for potential comorbidities (e.g. thyroid hormones and autoantibodies for active thyroid disease) or to exclude other diagnoses in the appropriate clinical context (e.g. skin biopsy for urticarial vasculitis).
With the exception of avoiding alcohol consumption, pseudoallergen-free or other food elimination diets should not be routinely recommended to patients for symptom control. In fact, IgE-mediated food allergy is rarely an underlying cause of urticaria.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Welcome to 3P: Pills, Pearls, and Patients where we will discuss current events in medicine, stories from real patient-physician encounters, and gain insight into what it's like being a physician in today's society.
Please note that while the first episode is available to listen to without registration, accessing additional episodes will require you to subscribe and log in.
Hello and welcome to the next episode of 3P, Pills, Pearls and Patients. I'm your host, Dr. Marina Malak. And today is part two of our series on Basically Back Pain.
...
0
No applauses yet
Dr. Marina Malak is a family physician in Mississauga, Ontario and a lecturer and faculty member at the University of Toronto. She is actively involved in medical advocacy, and is a board member of the Mississauga Primary Care Network. She is also a member of the National Committee of Continuing Professional Development at the College of Family Physicians of Ontario, and a member of the Research Ethics Board at Trillium Health Partners.
She is passionate about patient care; medical education; and promoting mental, physical, and emotional wellness. She enjoys reading, writing, public speaking, puzzles, doodling in her bullet journal, and creating drawings on Procreate.
RS: Hello and welcome to another episode of the Medical Narratives podcast. I'm Regina Starr and today we will delve into the topic of Frailty in the Elderly. Frailty among the elderly presents a multifaceted challenge to both society and society at large. As a medical condition, it signifies a state of vulnerability, often resulting from age related declines in physical and mental health. This condition places a significant burden on health care systems, increasing hospitalizations and health care costs.
Moreover, frail individuals may experience reduced quality of life and increased dependance on caregivers. Societally, addressing frailty necessitates reconfiguring health care systems to provide better support for older adults and promoting preventative measures through healthier lifestyles. The challenge of frailty underscores the pressing need for a comprehensive, age sensitive approach to elderly care. To discuss this topic, we sat down with Dr. Michael Gordon, a well-known geriatrician specialist and the host of the Medical Narratives podcast.
RS: Hi Michael.
MG: Hi. Good morning.
Please note, that to access this episode in full instead of the teaser available just below you would need to login.
Dr. Michael Gordon recently retired after a fulfilling career as a geriatrician that spanned 56 years, 44 of which he spent working at the Baycrest Center in Toronto. He is Emeritus Professor of Medicine at the University of Toronto. Dr. Gordon is a recognized ethicist and a thought leader on all topics of care of the elderly and end-of-life decisions. Currently, Dr. Gordon provides part-time professional medical consulting mainly in the domain of cognition and memory loss.
Welcome to Inside Radiology: A Primary Care Perspective where we explore the world of radiology and its applications in primary care.
Please note that while the first episode is available to listen to without registration, accessing additional episodes will require you to subscribe and log in.
Welcome back to another episode of Inside Radiology: A Primary Care Perspective podcast. I'm Dr. D'Arcy Little, your host, a community radiologist with a background in primary care. In today's episode, we are looking at abdominal pain imaging.
...
0
No applauses yet
Welcome to Inside Radiology: A Primary Care Perspective podcast! I'm Dr. D'Arcy Little, your host. As a community radiologist and former family physician, I'm passionate about empowering primary care doctors with the knowledge and insights they need. With my unique perspective, I aim to bridge the gap between primary care and radiology, presenting the complexities of radiology in a way that resonates with you. My goal is to equip you with tools to enhance patient care and decision-making. Join me on this educational journey as we explore the world of radiology, tailored for primary care physicians like you. Together, let's elevate primary care radiology.
1 Faculty of Medicine, University of British Columbia, Vancouver, British Columbia, Canada. 2Department of Pediatrics, Department of Dermatology and Skin Sciences, University of British Columbia, Vancouver, British Columbia, Canada.
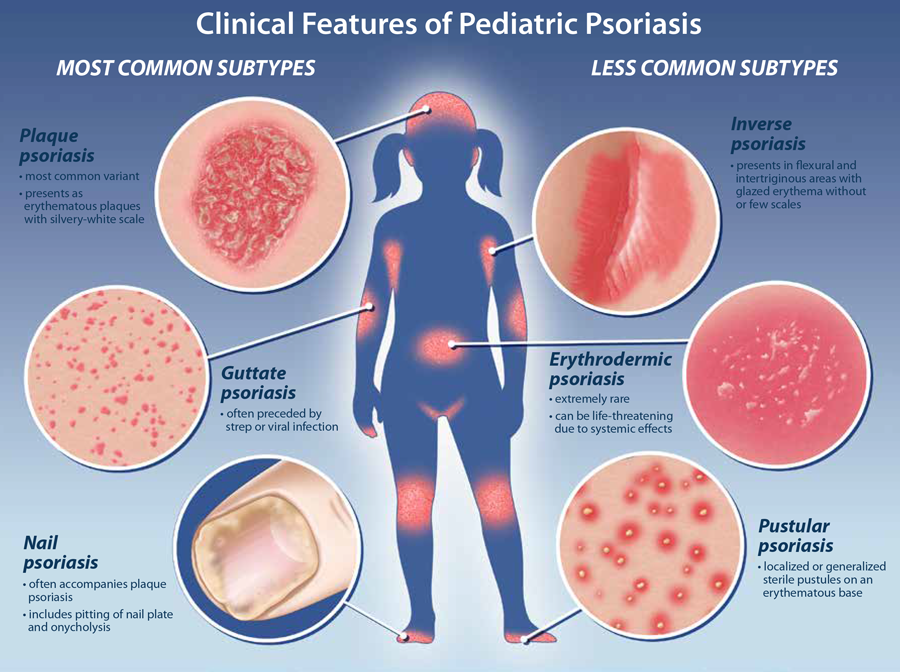
Abstract: Psoriasis is a chronic inflammatory skin disease that affects up to 1.4% of children (aged <18 years) with a strong genetic predisposition and is mediated by dysregulation in the crosstalk between the innate and adaptive immune responses. It can have significant impact on quality of life for many patients. There are various subtypes of psoriasis with plaque psoriasis being the most common presentation in both adults and children. Pediatric psoriasis is primarily a clinical diagnosis. With the advent of biologics, the treatment landscape for pediatric psoriasis has shifted and encompasses diverse modalities of therapeutics, including topical and systemic treatments, as well as phototherapy.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
Psoriasis affects the pediatric population and is associated with negative effects on quality of life and psychological impairments.
Lesions of pediatric plaque psoriasis may be thinner, smaller, more macerated than those classically in adult and present more commonly on the scalp, face, intertriginous areas, and extremities (flexural surfaces for younger children and extensor surfaces for older children).
Psoriasis is not an isolated condition and is correlated with higher rates of myocardial infarction, diabetes mellitus, hypertension, obesity, arthritis and liver disease.
In mild to moderate cases of psoriasis, topical therapies with a short course of corticosteroids and/or vitamin D analogue are first-line. In moderate to severe cases, narrowband UVB phototherapy, systemic agents, such as methotrexate, and biologics should be considered.
Pediatric patient should be assessed for risk factors for associated comorbidities.
A history of preceding streptococcal or viral infection can be suggestive of guttate psoriasis, which is more common in children than adults.
Approach to treatment should be guided by the extent and severity of disease, which can be quantified by BSA, the PASI score and quality of life index surveys.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Hello there. It's a pleasure to meet you all. My name is Alykhan Abdulla, and I am the co-host of Med Talks: Beyond the White Coat. This is our very first podcast. I'm actually very excited to participate in it with you and also share our surprising guest. Well, let me tell you a little bit about what our intention is, and then it'll be a lot easier when I introduce our guest.
Please note that while the first episode is available to listen to without registration, accessing additional episodes will require you to subscribe and log in.
00;00;00;00 - 00;00;44;05 AA: Hello there. It's a pleasure to meet you all. My name is Alykhan Abdulla, and I am the co-host of Med Talks Beyond the White Coat. This is our very first podcast, and I am excited. I am beyond excited to participate in this with you and to share our surprising guest. But let me tell you a little bit about what the intention of Med Talks is, and it'll be a lot easier when I introduce our guest.
00;00;44;07 - 00;01;12;15 AA: Med Talks Beyond the White Coat is an opportunity to understand about leadership. And we're going to meet some incredible leaders and you will get to hear from them about their stories and what they've gone through to achieve their leadership role, their struggles, their challenges, their successes, and the things that they learned along the way to make sure that they were prepared and ready and confident to move forward in their leadership role.
00;01;12;17 - 00;01;41;26 AA: And more importantly, you're going to hear advice. Advice that they want to share. Advice to help others who are motivated to follow in their footsteps, to climb up on their shoulders and move forward to their next leadership challenge. So with that, I would like to introduce our very first podcast guest, Dr. Kathleen Ross. Dr. Kathleen Ross is the president of the Canadian Medical Association.
00;01;41;28 - 00;02;08;16 AA: She grew up in small town Port Coquitlam, British Columbia. She's a mother of two and she's been married for 35 years. In addition to doing clinical work in family medicine, comprehensive family medicine, she also has done work in obstetrics and surgical assisting during this entire time period. She was also previously the President of the Doctors of B.C., which is a feat upon itself.
00;02;08;19 - 00;02;38;20 AA: It's British Columbia's provincial Medical Association for its 15,000 doctors. And in addition to that, she's been involved in health care and health care policy and led many grassroots improvements. Those include the chair of the Fraser Northwest Division of Family Practice and the president of the medical staff of the Royal Columbian Hospital. She's a founding member of the Doctors of B.C. Diversity and Inclusion Advisory Group.
00;02;38;22 - 00;03;07;00 AA: She's had the opportunity to be the lead in regards to anti-racism and unconscious bias. She's helped elevate all kinds of leaders in all kinds of positions using her skill sets of diversity and thoughtfulness. She was involved in the physician quality improvement. She chairs the CMA administrative burden and working Group and participates in the McMaster National Fellows Program for Health Care Leadership.
00;03;07;02 - 00;03;28;26 AA: And this is the part that I'm hoping that we can get into today. I'm hoping we can talk about her volunteerism because it was her service in her past that has been the absolute cornerstone for the type of leadership that she brings, authentic and honest. She worked in the Andean regions of Peru, and she speaks some of their languages, believe it or not.
00;03;28;29 - 00;03;47;14 AA: She's also helped and spent time with the Girl Guides of Canada. And before that, she was honoured with the Terry Fox Wall of Fame in Coquitlam in 2019. With that, I'm excited to introduce you. Dr. Kathleen Ross. Dr. Ross, how are you?
00;03;38;16 - 00;03;38;23 KR: Very good. How are you?
...
0
No applauses yet
Alykhan Abdulla, BSC, MD, LMCC, CCFPC, DipSportMed CASEM, FCFCP, CTH (ISTM), CCPE, Masters Cert Phys Leader, ICD.D
is the Medical Director of The Kingsway Health Centre, The Kingsway Travel Clinic, and The Kingsway Cosmetic Clinic.
He is also the Assistant Professor at the University of Ottawa Faculty of Medicine and Academic Clinical Professor
at the University of Ottawa Faculty of Nursing. In addition he is the Director of UOttawa Undergraduate Medical
Education Leadership Development Curricula. Dr. Abdulla is the Editor in Chief Journal of Current Clinical Care
Sports Medicine section. He is the Board Director Bruyere Continuing Care, ESO-OHT Primary Care Table, Ontario
Medical Foundation, College of Family Physicians of Canada, 700 Sussex Drive Board (OCLCC 713), The Rideau Club
Finance & Audit and Past Chair Section of General and Family Practice Ontario Medical Association.
Moiz Lakhani, BHSc graduate from McMaster University and current medical student at the University of Ottawa,
co-hosts the Med Talks: Beyond the White Coat podcast. A 2021 Cansbridge fellow, Moiz has spoken at the UN HQ, Youth Assembly
Conferences, and WISE in Qatar. He's also a 2022 Diana Award recipient, the highest honor for youth in social action and
humanitarian work.