Simone Pomati, MD, PhD, Centre for Research and Treatment on Cognitive Dysfunctions, Institute of Clinical Neurology, Department of Clinical Sciences, Luigi Sacco Hospital, Milan, Italy.
Francesca Clerici, MD, PhD, Centre for Research and Treatment on Cognitive Dysfunctions, Institute of Clinical Neurology, Department of Clinical Sciences, Luigi Sacco Hospital, Milan, Italy.
Stefano Defendi, MD, Centre for Research and Treatment on Cognitive Dysfunctions, Institute of Clinical Neurology, Department of Clinical Sciences, Luigi Sacco Hospital, Milan, Italy.
Silvia Bovo, MD, Centre for Research and Treatment on Cognitive Dysfunctions, Institute of Clinical Neurology, Department of Clinical Sciences, Luigi Sacco Hospital, Milan, Italy.
Claudio Mariani, MD, Chair of Clinical Neurology, University of Milan; Centre for Research and Treatment on Cognitive Dysfunctions, Institute of Clinical Neurology, Department of Clinical Sciences, Luigi Sacco Hospital, Milan, Italy.
Frontotemporal dementia (FTD) is a progressive condition characterized by atrophy of the frontal and/or temporal lobes. Three main clinical syndromes have been described (behavioural variant, progressive nonfluent aphasia, and semantic dementia). The symptoms reflect the anatomical distribution of the pathological changes rather than the precise histological subtype. Frontotemporal dementia is a genetically complex disorder with a strong likelihood of inheritance, mainly transmitted as an autosomal dominant trait. Mutations in microtubule associated tau protein and progranulin have been reported in several families affected by FTD. The treatment is directed to the control of the behavioural disturbances through pharmacological and nonpharmacological approaches.
Key words: frontotemporal dementia, semantic dementia, progressive nonfluent aphasia, neuropsychology, progranulin.

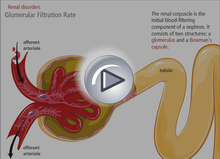 Chronic kidney disease (CKD) is increasingly common among older adults. In the older individual, the presence of CKD is predictive of cardiovascular death, increased all- cause mortality, and progression to end-stage renal disease and the need for dialysis. Early identification of these high-risk individuals may prevent or delay such adverse outcomes. The Canadian Society of Nephrology (CSN) released a position statement in September 2006 suggesting that screening be limited to those at high risk. We recommend that clinicians follow the CSN algorithm for screening for CKD among older adults.
Chronic kidney disease (CKD) is increasingly common among older adults. In the older individual, the presence of CKD is predictive of cardiovascular death, increased all- cause mortality, and progression to end-stage renal disease and the need for dialysis. Early identification of these high-risk individuals may prevent or delay such adverse outcomes. The Canadian Society of Nephrology (CSN) released a position statement in September 2006 suggesting that screening be limited to those at high risk. We recommend that clinicians follow the CSN algorithm for screening for CKD among older adults.