Abstract: Cervical spine injury can have life-changing consequences. At every stage of injury, we can intervene to meaningfully change patients' outcomes. On the field, a high index of suspicion is critical. Spinal immobilization prevents secondary injury, but immobilization, particularly use of a hard board, must be kept to a minimum. In the trauma bay, perfusion of the spinal cord is a priority to help prevent secondary spinal cord injury. This means addressing any cause of hypotension and understanding how to manage neurogenic shock. In the spinal-cord injured patient, hemodynamic management is an important adjunct.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
1. Minimize time in rigid immobilization as much as feasible.
2. Spinal shock is temporary flaccid paralysis and loss of reflexes. You cannot give a prognosis for a spinal cord-injured patient in spinal shock.
3. Recognize patients with stiff spines (such as in ankylosing spondylitis) and immobilize them in their natural position of comfort to avoid secondary injury.
4. What we can do to improve neurologic outcomes in spinal cord injury: Maintain spinal cord perfusion through oxygenation and blood pressure management, avoid secondary injury through immobilization, and facilitate early surgical decompression (<24hr)
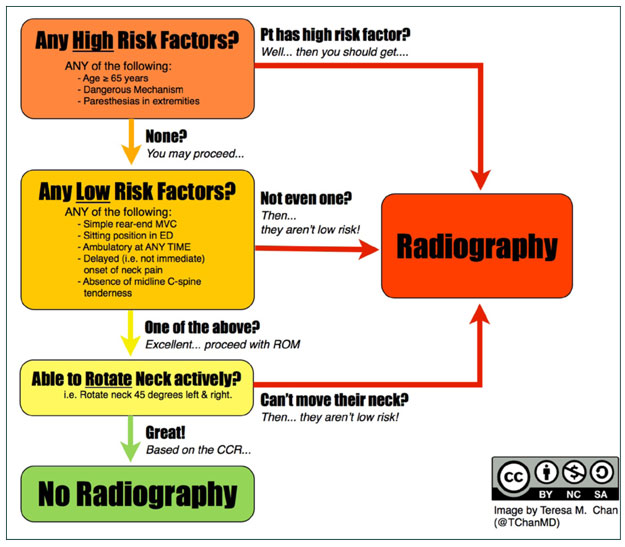
1. The Canadian C-spine Rule is the preferred algorithm to clear the cervical spine after trauma.
2. X-rays are not sufficient to rule out cervical spine injury. CT scan is the gold standard.
3. Neurogenic shock is a distributive syndrome characterized by the triad of hypotension, bradycardia, and peripheral vasodilation. First line treatment is fluid resuscitation, then vasopressors.
4. Patients with stiff spines (ankylosing spondylitis or DISH) have high rates of spine fractures and non-contiguous injuries. Full spine CT scans should be obtained.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.
Vadim Beletsky, MD, PhD, Senior Stroke Fellow, Department of Clinical Neurological Sciences, London Health Sciences Centre, London, ON.
Clinical presentation of cervical arterial dissection is highly variable, but headache or neck pain is frequently observed. Both invasive and noninvasive imaging are used to confirm the diagnosis but noninvasive techniques overshadow traditional digital subtraction angiography (DSA), which should be reserved for cases where invasive procedures are planned. In spite of the accumulated clinical, diagnostic, and etiological data on cervical arterial dissections in recent years, there is no evidence to support the use of a particular class of antithrombotic agents in these patients. Different pathophysiology of brain ischemia in acute and chronic states of dissection may advocate different treatment strategies, including surgical. There are also no imaging follow-up guidelines, both in terms of frequency and modality, further affecting secondary stroke prevention uncertainties.
Gynaecologic Cancers Remain Leading Cause of Cancer-related Deaths in Women
Teaser:
Nariman Malik, BSc
Gynaecologic cancers remain a leading cause of cancer-related deaths in Canadian women. The three malignancies focussed on in this article, endometrial cancer, ovarian cancer and cervical cancer, have good prognoses if they are detected in their early stages. As such, it is of utmost importance that primary health care physicians be aware of Canadian guidelines for detecting these conditions and their limitations.
Endometrial Cancer
When diagnosed early, endometrial cancer is highly treatable and has a high survival rate. Stage I, grade I endometrial cancer has a five-year survival rate of 98%. This type of cancer most often presents as post-menopausal vaginal bleeding early in the course of the disease. Any woman who presents with unexplained post-menopausal bleeding should undergo endometrial assessment which can lead to early detection and improve the chances for a cure.
Detection
To identify women at risk of developing endometrial cancer, the progesterone challenge test can be used. In the United States, it had been recommended that all post-menopausal women should undergo this test at each annual examination. There are currently no Canadian recommendations regarding this test.