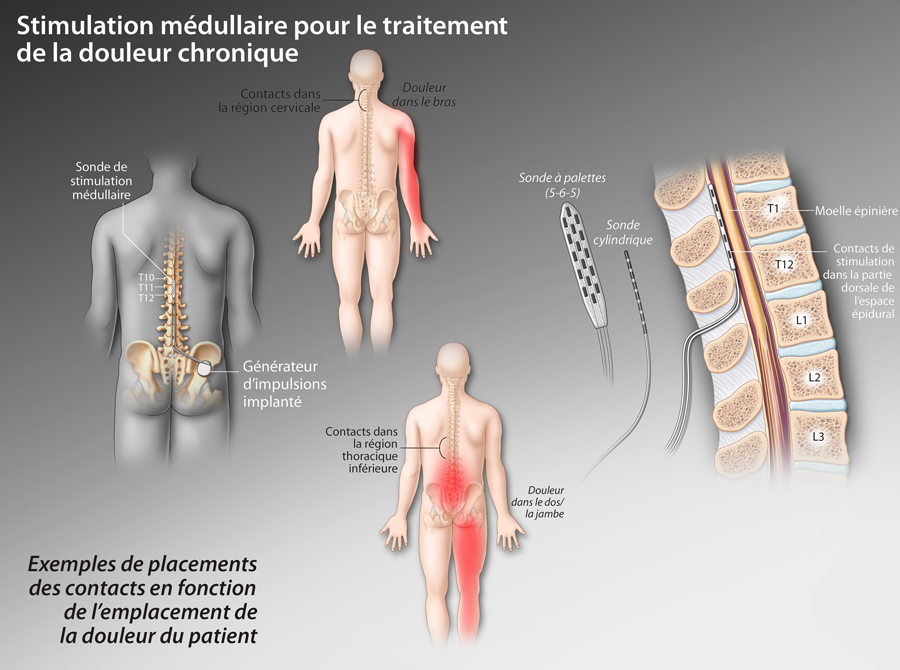
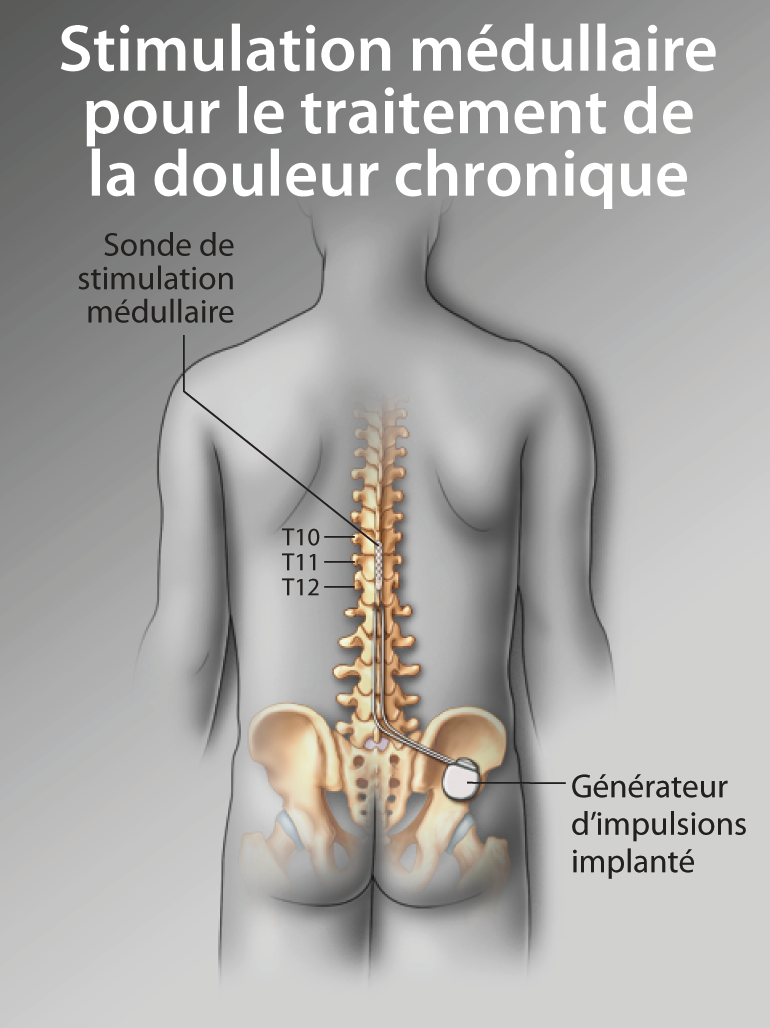
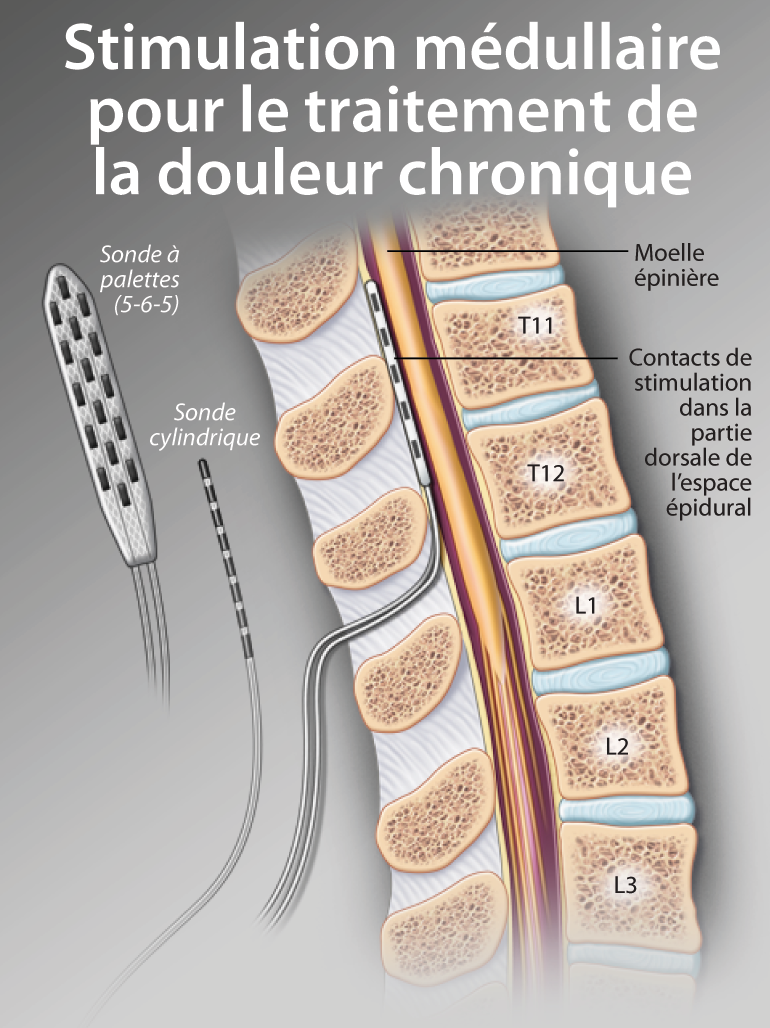
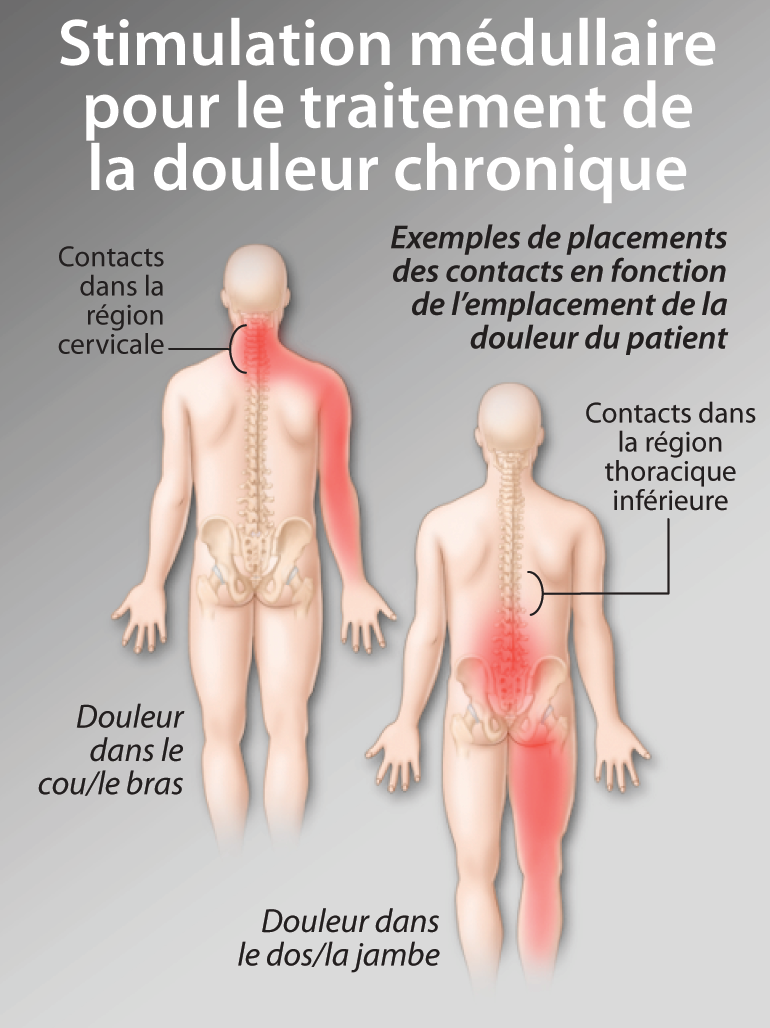
Neurostimulation médullaire : une approche thérapeutique de la douleur sous-utilisée et mal reconnue


Disclaimer:
Cet article a été publié dans le cadre de Prise en charge de la santé de votre patient âgé : thérapies qui pourraient aider à améliorer la qualité de vie ressource FMC.
Ce document a reçu un appui dans le cadre d’une subvention pédagogique de Medtronic Canada Ltée.