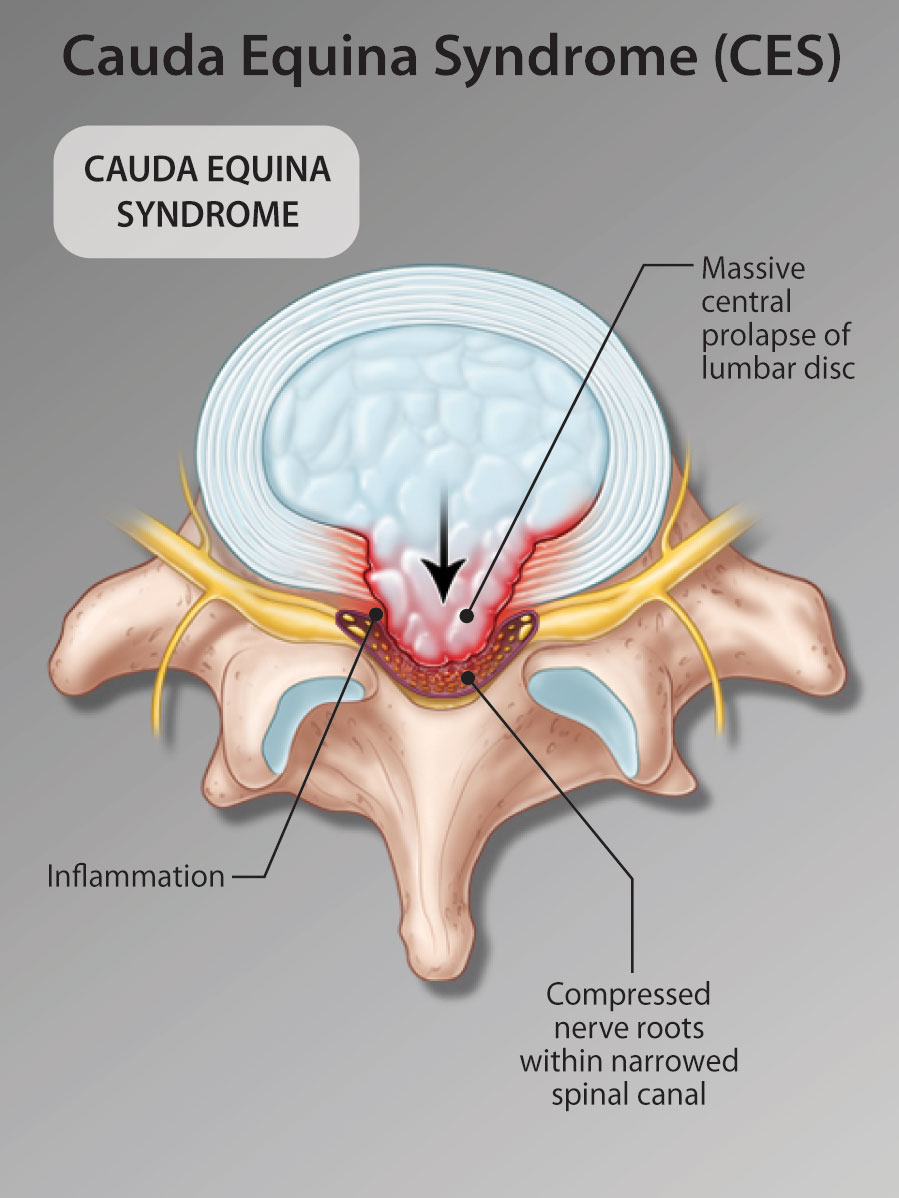
Abstract: Cauda Equina Syndrome (CES) is a rare progressive syndrome of pain and neurological deficits below the waist caused by massive central lumbar disc prolapse. The most common clinical presentation is highly variable with multifocal mixed polyradicular deficits. Loss of bladder and/or bowel control can be subtle and is frequently not the patient' chief complaint. These symptoms must be aggressively sought by the assessing physician. While delays of a few hours in the diagnosis and management may not be deleterious, definitive lumbar MRI imaging and (if positive) surgical care referral are emergent.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
The CES patient often presents with rapidly escalating, poorly controlled pain. There may be daily or even more frequent physician visits.
While standing, the CES patient commonly adopts a "sciatic scoliosis": forward bending at the waist and leaning to either side as they attempt to decompress themselves. They may limp or need walking aids. These features help distinguish them from drug-seekers or malingerers.
Since patients are distracted by extreme pain, they may not reliably volunteer a history of bladder/bowel disturbance.
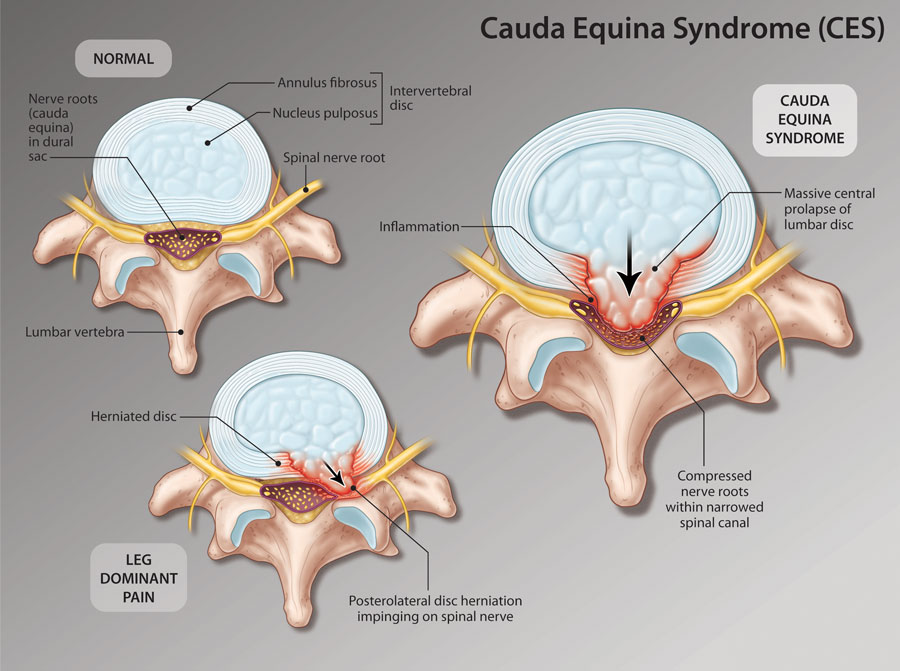
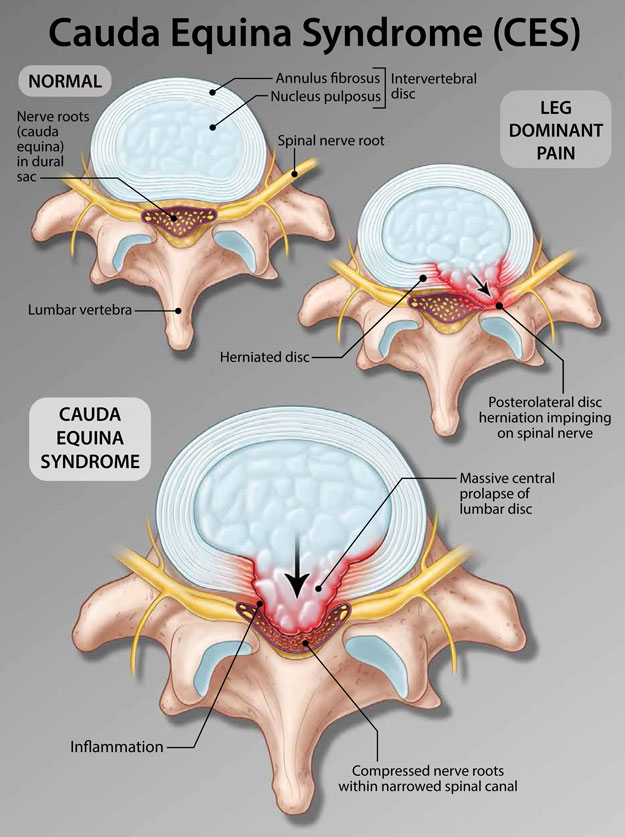
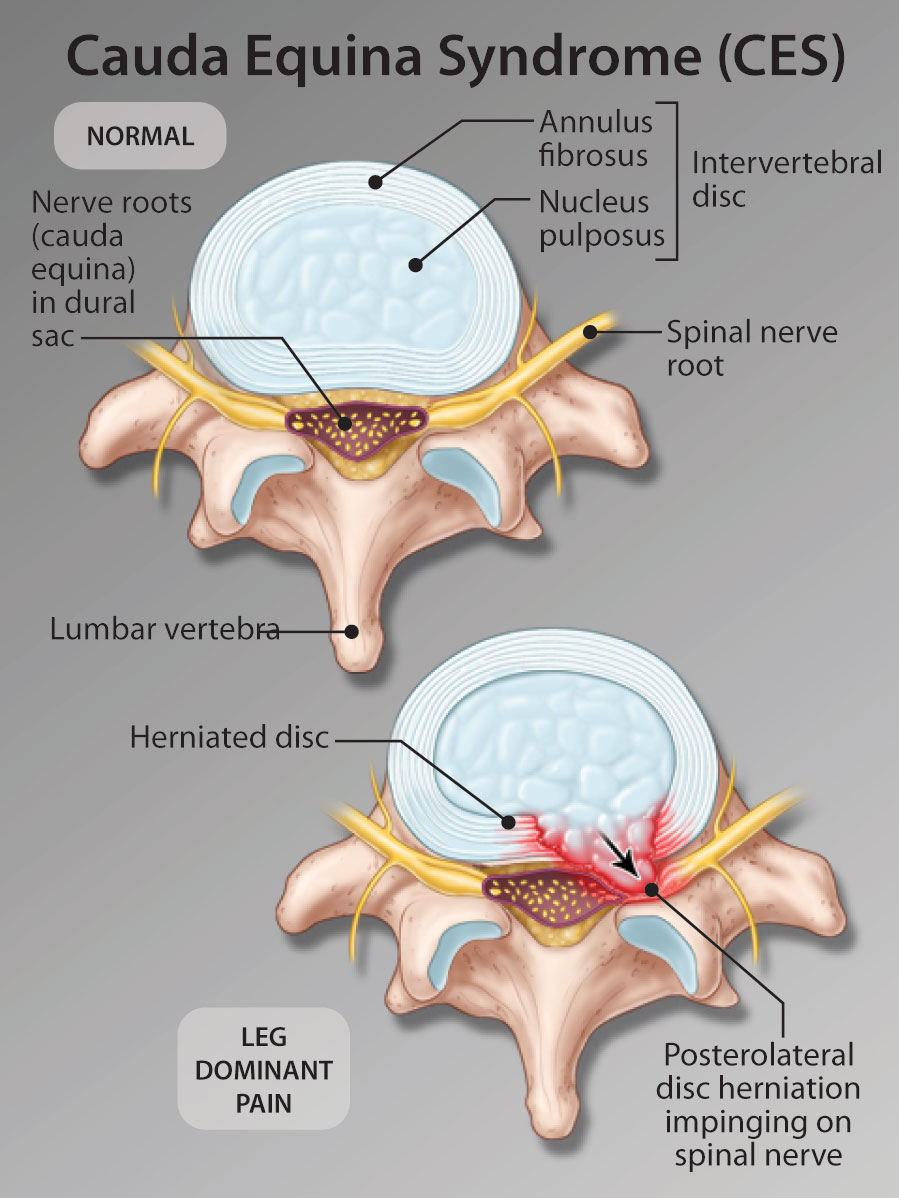
Cauda Equina Syndrome is an acute or subacute pathology caused specifically by massive central prolapse of a lumbar disc. Decompensation lumbar spinal stenosis is not Cauda Equina Syndrome.
Cauda Equina Syndrome most commonly presents with complaints of back or leg pain. These differ from common sciatica in being rapidly progressive, difficult to control with analgesics and often associated with considerable locomotor impairment.
The neurological examination in Cauda Equina Syndrome most commonly finds a mixed pattern of incomplete polyradicular deficits in the distribution of multiple lumbar and sacral nerve roots involving either of the legs and/or the saddle (perineum). The classically described complete flaccidity with loss of all motor control from the waist down is extremely rare.
Patients presenting with CES will not commonly volunteer complaints of incontinence or urinary retention as they are often overwhelmed by the magnitude of their pain. The assessor must specifically ask about bowel/bladder function and when indicated, test these by bladder scanning or catheterizing and a digital rectal examination.
As a rapidly evolving syndrome of neurological deterioration, CES warrants emergent imaging investigation and referral. Although the literature is not precise on the critical time point, it is widely accepted that patients should receive surgical intervention within 24 to 48 hours.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.