The neurosciences seem always to have been a strong point of Canadian medicine, from both a clinical and a research perspective. Montreal, with its Neurological Institute, has long been internationally renowned. In fact, the day I wrote this editorial, there was an article in the Globe & Mail announcing that a famous American neuroscientist was moving to the MNI because he felt there were greater opportunities there than in his current position in New York City! Clearly, Montreal remains at the forefront of neuroscience research, but it is no longer the only excellent Canadian venue. Several universities across the country have made neuroscience research a priority, and most have excellent multidisciplinary research enterprises. In my University (Toronto), there are numerous outstanding investigators. Don Stuss heads a group at the Baycrest Centre for Geriatric Care that has done groundbreaking work on frontal lobe function. Peter St George-Hyslop at the Centre for Research in Neurodegenerative Diseases (CRNDs), is an international authority on the genetics and molecular biology of Alzheimer disease. There is outstanding work being done on brain tumours, dementia, stroke, epilepsy and other neurological conditions.
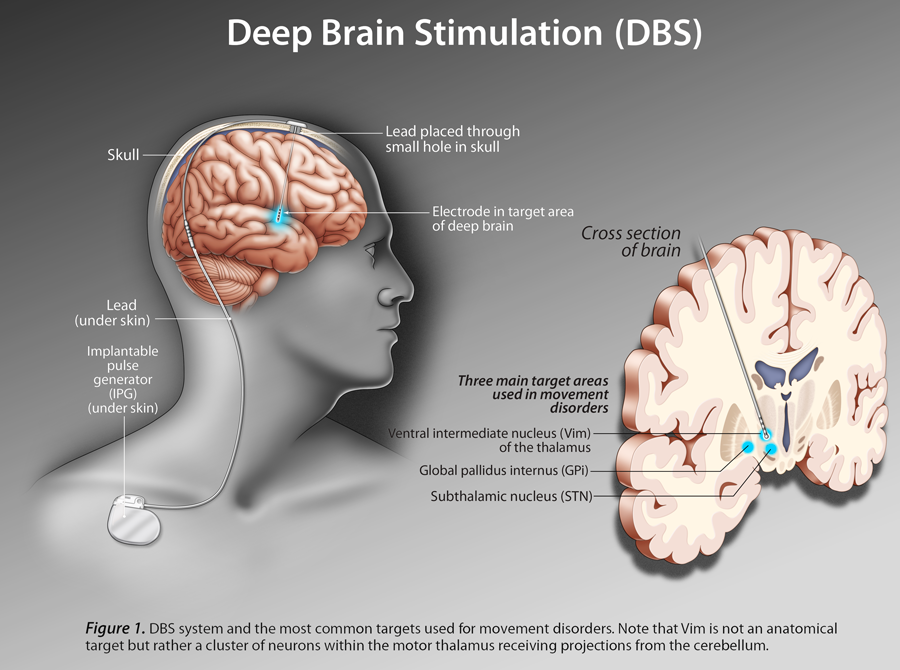
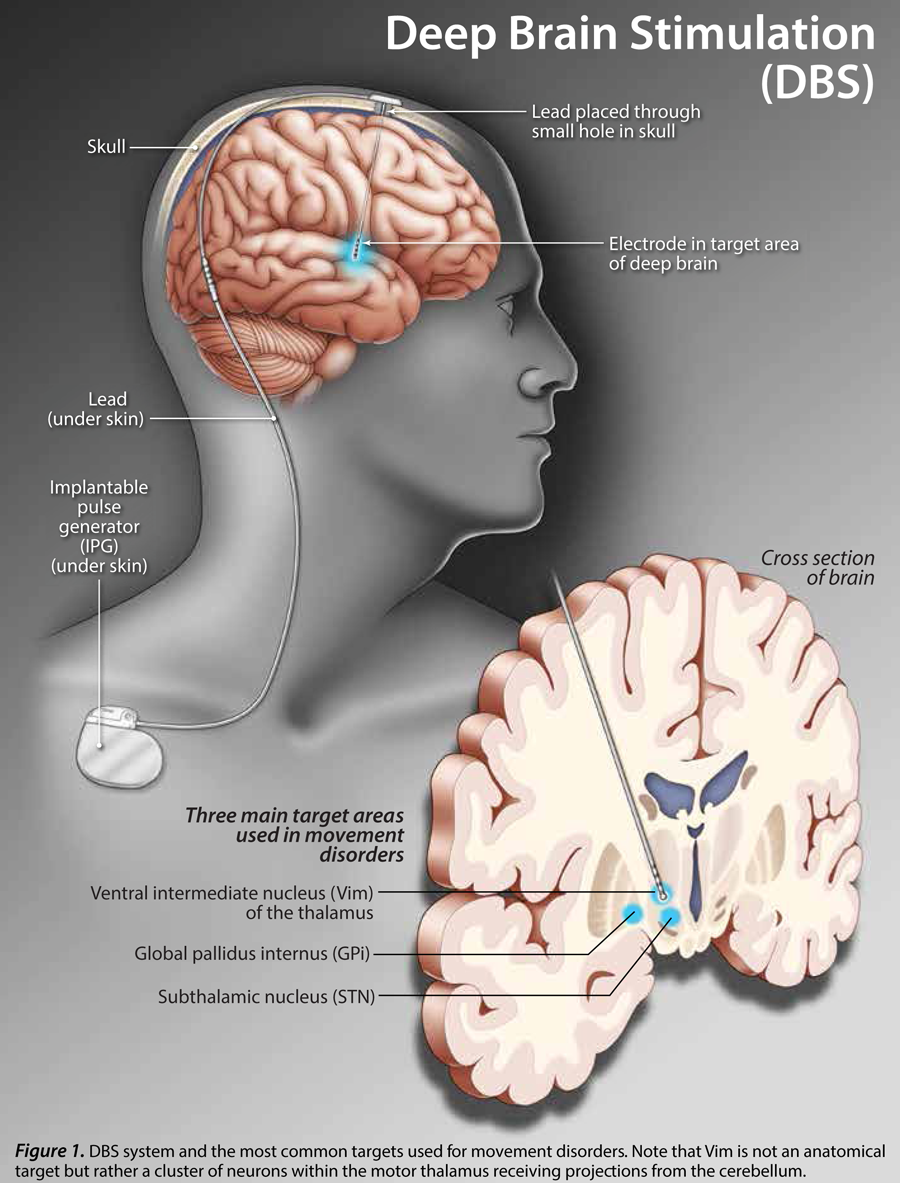
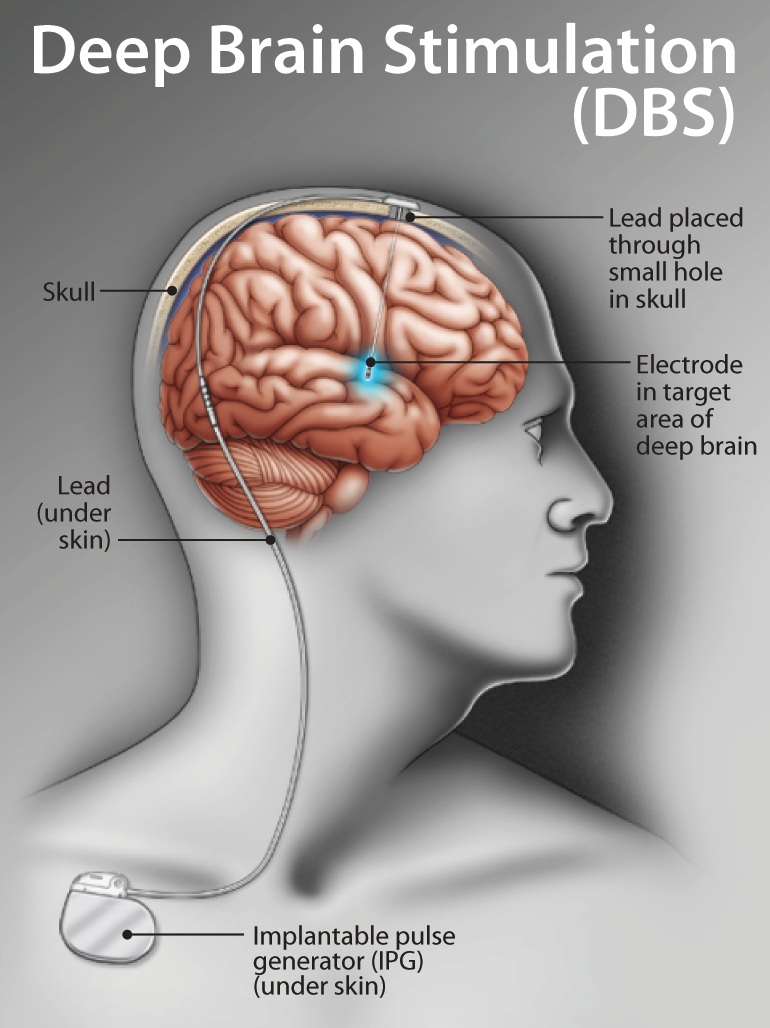
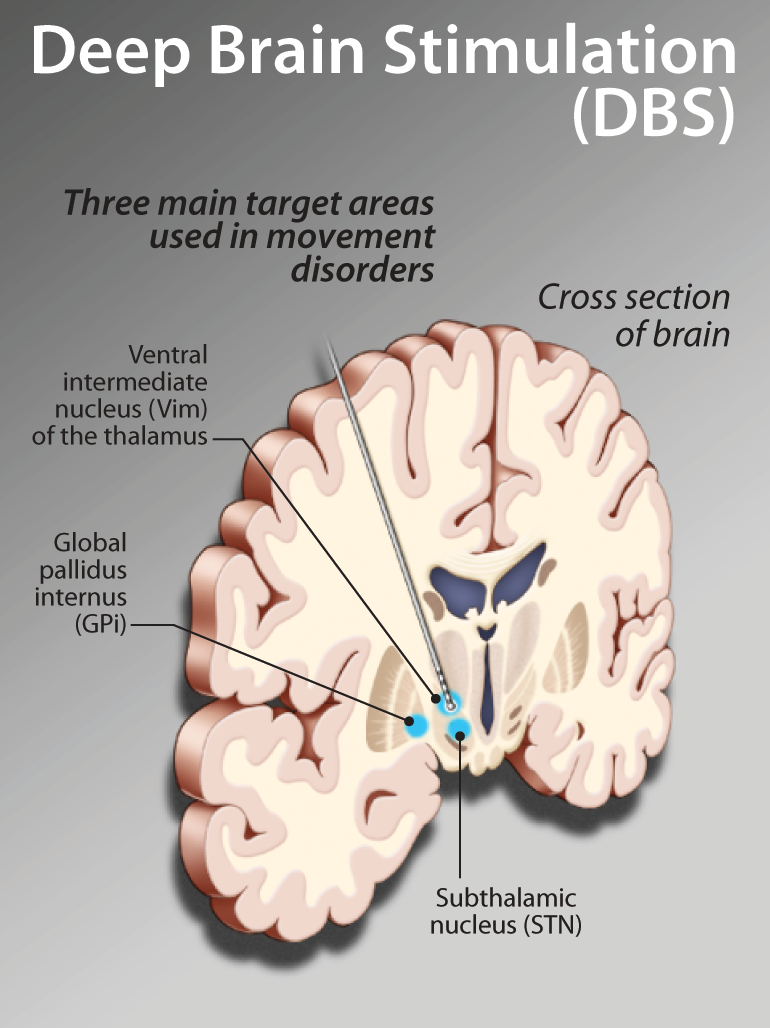
However, in Canada there seems to be particular strength and depth in the field of movement disorders. Although we have one article from the United Kingdom (Hallucinations in Patients with Parkinsonism, by Dr. Burn and Professor McKeith), it is a relatively easy task to find Canadian experts in all facets of the movement disorders. One Canadian, Dr. Ali Rajput from Saskatoon, has made an incredible contribution by his careful clinical-pathological correlations in Parkinson's disease (PD). He is considered one of the world's leading clinicians in the care of patients with PD. He and Dr. Alex Rajput (his son) have written an article on how to differentiate Parkinsonian Dementia from Alzheimer disease, as well as on its management. We have an article on diagnosing and managing depression in Parkinson's disease by Dr. Mandar Jog, the director of the Movement Disorders Program at the University of British Columbia. Zhigao Huang and Robert Tsui from the Pacific Parkinson's Research Centre at UBC discuss COMT inhibition in Parkinson's disease. Robert Chen and Daniel Sa, from the University of Toronto, give an update on advances in therapeutic strategies for Parkinson's disease, including pallidotomy and deep brain stimulation.
Of course, Parkinson's Disease is not the only movement disorder. D'Arcy Little, a frequent contributor to this journal, discusses the epidemiology, presenting features, diagnosis and treatment of Huntington's Disease. In other articles, Deborah Hebert from the Toronto Rehabilitation Institute and the University of Toronto discusses limb apraxia from a clinical perspective. Dr. Madhuri Reddy has written an article on the natural history of long-term care clients. Dr. Robert Teasell from the University of Western Ontario, and one of Canada's leaders in stroke rehabilitation, shares his knowledge of the area with us. As well, the Regional Geriatric Programs of Ontario have submitted an educational module on Driving & Dementia. Enjoy!
Next month, by popular demand, the issue will focus on skin disorders in the elderly. Be sure not to miss it!