1PGY4 Dalhousie Neurosurgery Program, Dalhousie University, Halifax, NS. 2Professor, Department of Surgery (Neurosurgery), Faculty of Medicine, Vice-Chair and Director of Research , Division of Neurosurgery, Dalhousie University.
Abstract: Inflammatory spondyloarthropathies produce synovitis of the spinal joints in rheumatoid arthritis (RA), or enthesitis in ankylosing spondylitis (AS). In RA, progressive disease leads to synovial destruction, ligamentous laxity, pannus formation and deformity. In AS progressive enthesitis results in ascending ossification, kyphotic deformity and rigidity which increase the risk of fracture. Although pain is the common presentation, spinal cord compression can produce neurological deficits. Although the need for surgery has decreased with the advent of new disease altering drugs, there remains a number of indications when surgical consultation remains important.
Key Words: Spondyloarthropathy and spondyloarthritis, Synovium and synovitis, Enthesis and enthesitis, Pannus.
Members of the College of Family Physicians of Canada may claim MAINPRO-M2 Credits for this unaccredited educational program.
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.
1. Inflammatory arthritis from multiple etiologies may affect the spine with different patterns and pathophysiology.
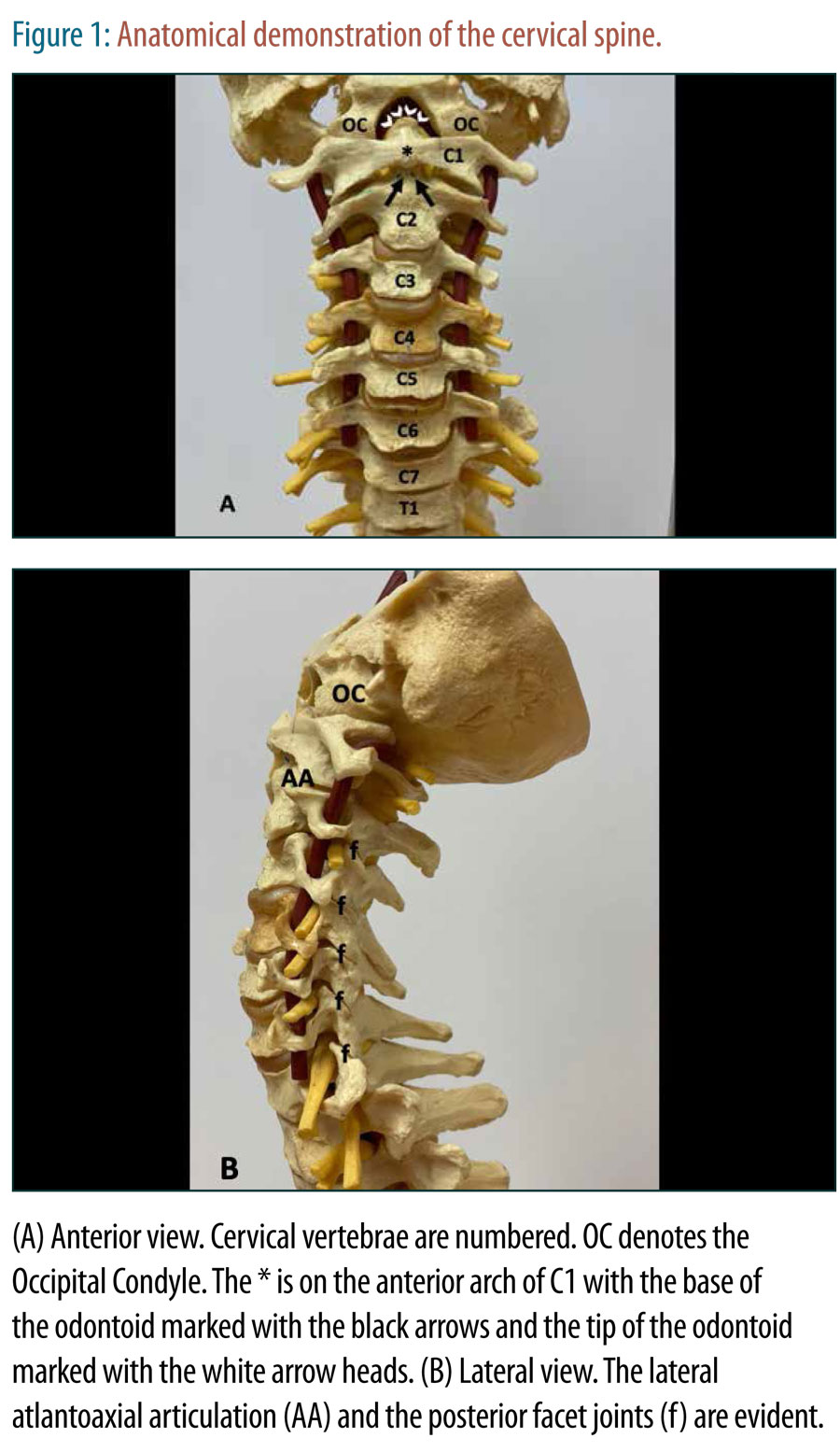
2. Rheumatoid arthritis is a disease of synovial inflammation and in advanced disease leads to synovitis within the atlanto-dental articulation and the facet joints of the spine.
3. If left untreated atlantoaxial subluxation, cranial settling and pannus formation may lead to spinal cord and lower medullary compression.
4. Seronegative arthropathies leads to an enthesitis of the spine, usually starting in the sacroiliac spine and ascending with progressive ossification.
5. As a consequence of pathological alteration of the spine biomechanics, trauma in the setting of ankylosing spondylitis leads to different fracture patterns with a high chance of instability even after minimal trauma.
1. Early and adequate treatment of rheumatoid arthritis can prevent advanced atlanto-axial disease, deformity and neurological injury.
2. Even minimal trauma to the spine in a patient with ankylosing spondylitis has a high risk of instability and neurological injury; detailed imaging is always warranted.
3. With the advent of modern disease modifying agents for the treatment of spondyloarthropathies, the requisite for surgery has decreased but there remain important indications.
To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app.