Basal Cell Carcinoma
Basal cell carcinoma (BCC) is a common, slow-growing malignant skin tumour that only very rarely metastasizes. The main subtypes of BCC are nodular, superficial, and sclerosing. The most important risk factors for the development of BCC include fair skin, extensive sun exposure as a child, past personal history of skin cancer, and advanced age. Basal cell carcinoma is the most common human malignancy, and its incidence is increasing worldwide. There are a number of different treatm ent modalities for BCC including topical therapies, cryotherapy, electrodesiccation and curettage, surgical excision, radiotherapy, and Mohs’ micrographic surgery. Treatment should be tailored to the individual situation, and advanced age does not typically alter the management choice or reduce the expectation of an excellent outcome, including cure.
Key words: basal cell carcinoma, nonmelanoma skin cancer, risk factors, epidemiology, treatment.
Introduction
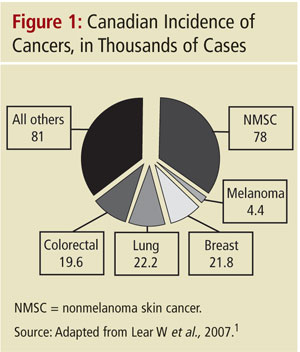
Basal cell carcinoma (BCC) is the world’s most common human cancer. Of the three major types of skin cancer, which also include squamous cell carcinoma (SCC) and melanoma, BCC accounts for approximately 70–80% of all skin cancers, while SCC accounts for 10–20% and melanoma 2–7%.1,2 BCC, SCC, and melanoma are distinct entities that do not transform into each other. Basal cell carcinoma is predominantly seen among fair-skinned individuals in middle to late life. In Ca nada, there are more than 78,000 cases of BCC and SCC per year, which roughly equals the incidence of lung, breast, and colorectal cancers combined (Figure 1). Incidence rates vary by geographical location, sun exposure, and skin type.
The highest incidence of BCC is observed where fair-skinned people inhabit regions with heavy exposure to ultraviolet (UV) light, such as Australia.3,4 Comparison data from across Canada, the U.S., and Australia have shown a continuous ste ady rise in the incidence of BCC—on average, 3–8% per year.5,6 Basal cell carcinoma most often develops on sun-exposed areas—80% occur on the head and neck7—but can occur anywhere on the body. Basal cell car cinomas are locally invasive tumours that are usually slow growing and only rarely metastasize.
A history of an otherwise-asymptomatic skin lesion that bleeds with little trauma (such as washing the face), heals, and then rebleeds is characteristic of BCC. If left untreated, the tumour may extend into cartilage and bone causing disfigurement. Mo rbidity is more often associated with tumour extension into a vital structure than from metastasis, which is rare (metastasis rates of 0.0028–0.55% have been reported).7
In BCC, genetic injury to cells in the lower epidermis and hair follicle is the inciting pathogenic event, followed by dysregulation in immune system controls and local protective mechanisms for stopping the spread. There is evidence that older skin i s at particular risk, not only due to a lifetime of genetic injury via UV damage, but also because local and systemic immune responses are less able to react to the threat. Older skin has been shown to have a reduced ability for repair of deoxyribonucle ic acid (DNA), lowered cell-mediated immune surveillance, and decreased barriers to tumour spread as aging weakens tissue planes.8
Risk Factors
The most notable risk factors for BCC are UV exposure and fair skin (Table 1). Intermittent intense UV exposure (especially blistering sunburns in childhood and adolescence) has been shown to correlate with an increased risk of BCC development.9, 10 This childhood exposure typically has a very long latency period, which explains the development of