Jagdish Butany, MBBS, MS, FRCPC, Department of Pathology, Toronto General Hospital, University Health Network; Department of Laboratory Medicine and Pathobiology, University of Toronto, Toronto, ON.
Gursharan S. Soor, BSc, Department of Pathology, Toronto General Hospital, University Health Network, Toronto, ON.
Adriana Luk, BSc, Department of Pathology, Toronto General Hospital, University Health Network, Toronto, ON.
Anna Woo, MD, FRCPC, FACC, Hypertrophic Cardiomyopathy Program, Division of Cardiology, Toronto General Hospital; Department of Medicine, University of Toronto,Toronto, ON.
Anthony Ralph-Edwards, MD, FRCSC, Division of Surgery, Toronto General Hospital, University of Toronto, Toronto, ON.
Heather Ross, MD, FRCPC, Department of Medicine, Division of Cardiology, University of Toronto, Toronto General Hospital, Toronto, ON.
Hypertrophic cardiomyopathy (HCM) is an uncommon disease with significant consequences. Since the 1950s, major strides in understanding its etiology and pathogenesis have led to improved management and patient survival. Hypertrophic cardiomyopathy is associated with various mutations in several cardiac sarcomeric genes. Due to the complications of HCM, such as left ventricular outflow tract obstruction, diastolic dysfunction, arrhythmias, increased risk of stroke, infective endocarditis, and, most importantly, sudden cardiac death, appropriate and timely diagnosis is critical. This review summarizes current knowledge about HCM and the most appropriate investigations for persons suspected of having HCM. Treatment strategies for the disease and its complications are presented briefly.
Key words: hypertrophic cardiomyopathy, cardiomyopathy, sudden cardiac death, older adults.

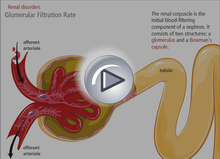 Chronic kidney disease (CKD) is increasingly common among older adults. In the older individual, the presence of CKD is predictive of cardiovascular death, increased all- cause mortality, and progression to end-stage renal disease and the need for dialysis. Early identification of these high-risk individuals may prevent or delay such adverse outcomes. The Canadian Society of Nephrology (CSN) released a position statement in September 2006 suggesting that screening be limited to those at high risk. We recommend that clinicians follow the CSN algorithm for screening for CKD among older adults.
Chronic kidney disease (CKD) is increasingly common among older adults. In the older individual, the presence of CKD is predictive of cardiovascular death, increased all- cause mortality, and progression to end-stage renal disease and the need for dialysis. Early identification of these high-risk individuals may prevent or delay such adverse outcomes. The Canadian Society of Nephrology (CSN) released a position statement in September 2006 suggesting that screening be limited to those at high risk. We recommend that clinicians follow the CSN algorithm for screening for CKD among older adults.