Marian Garfinkel, EdD, Medical Researcher and Adjunct Professor, Temple University, College of Health Professions, Department of Kinesiology; Medical Researcher, University of Pennsylvania, School of Medicine, Department of Rheumatology; Veterans Administration Hospital, Department of Rheumatology; Director, BKS Iyengar Yoga Studio of Philadelphia, Philadelphia, PA, USA.
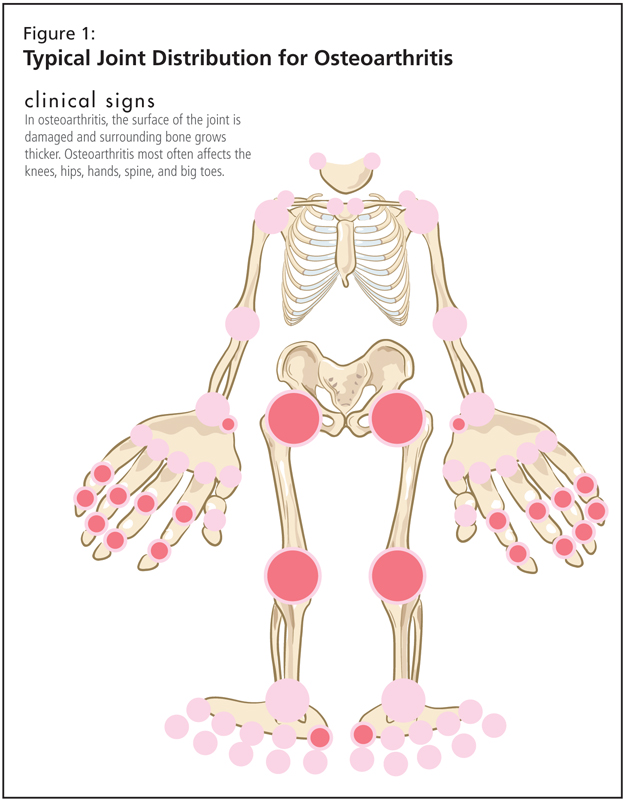
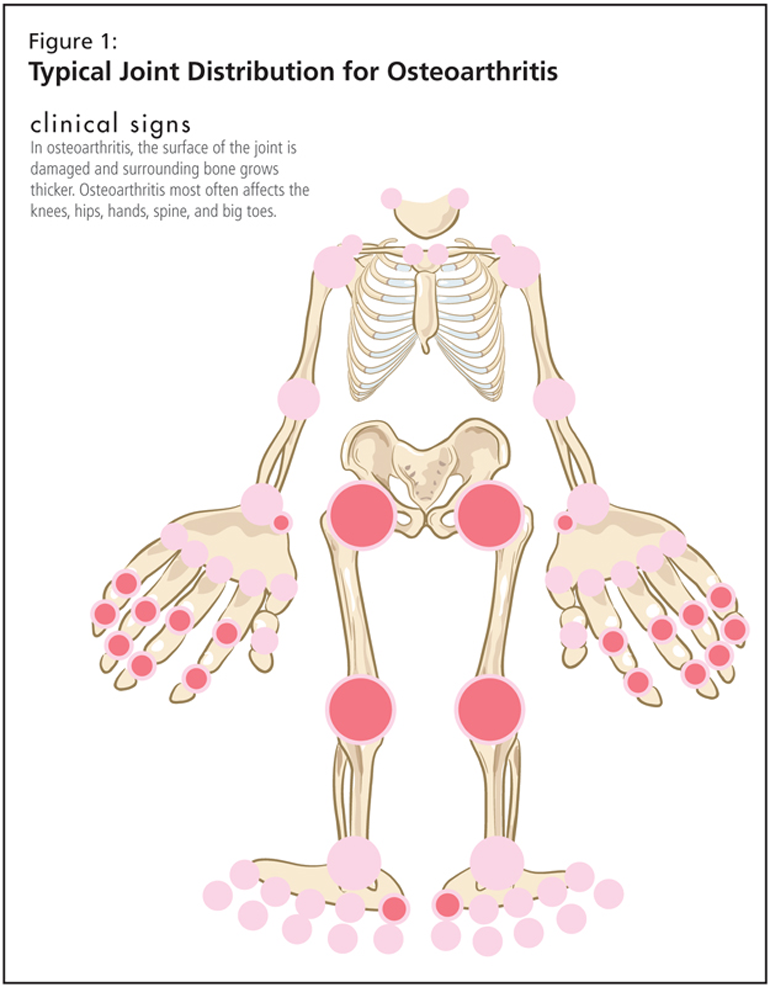
By broadening yoga’s application beyond stress-related ailments to include preventative and curative therapies, physicians today have an advantage in treating patients’ illnesses and disorders. Specifically, yoga therapy complements patients’ traditional medical treatment of osteoarthritis and other bone and joint disorders. Following anatomical guidelines, yoga teachers can adapt postures (asanas) to ensure patients’ organs, joints, and bones are aligned to achieve physiologic changes. Recent studies performed by this author assessing the effect of yoga therapy on rheumatic diseases, such as osteoarthritis, and repetitive strain injuries, such as carpal tunnel syndrome, showed that yoga therapy caused physiologic changes, relieved pain, and improved motion.
Key words: osteoarthritis, yoga, Iyengar, exercise, repetitive strain injuries.